Download
1 / 111
1.11k likes | 1.13k Vues
Explore the intricate structures and functions of the respiratory system, gas exchange processes, lung capacities, and the effects of ventilation-perfusion mismatch on oxygenation levels.

E N D
Chapter 21Control of Respiratory Function
Lung Functions • Gas exchange • Moves O2 into blood • Removes CO2 from blood • Barrier immunity • Regulates vasoconstricting substances • Bradykinin • Angiotensin II • Heparin
Conducting Airways • Move air into the lungs • Warm and humidify air • Trap inhaled particles
Respiratory Airways • Bronchioles • Alveoli • Gas is exchanged with the blood.
Question Which serous membrane lines the thoracic cavity? • Viscera pleura • Parietal pleura • Visceral mediastinum • Parietal mediastinum
Answer B. Parietal pleura Rationale: The organs and walls of the thoracic and abdominal cavities are covered with serous membranes. Visceral membranes cover the organ; parietal membranes line the cavity walls. The two membranes and the space between them allow for ease of movement. The thoracic cavity is lined by parietal pleura; the lungs are covered by visceralpleura.
Respiratory Muscles • Diaphragm • Accessory muscles of inhalation • External intercostals • Scalene • Sternocleidomastoid • Accessory muscles of exhalation • Internal intercostals • Abdominal muscles
Question True or false? During inhalation, the diaphragm contracts and flattens.
Answer True Rationale: The diaphragm is the main muscle of inhalation/inspiration. During inhalation, the diaphragm contracts and flattens (it moves downward in order to accommodate the volume of air you are taking in, allowing space for the lungs to expand). During exhalation, the diaphragm relaxes and moves back up.
Compliance • How easily lungs can be inflated depends on • Elastin and collagen fibers • Water content • Surface tension
Scenario • A man’s lungs were damaged during a fire, and he developed severe respiratory distress. • The doctor said smoke inhalation had caused an inflammation of his alveoli and destroyed some of his surfactant. Questions: • What happened to his lung compliance? • Why was he given positive-pressure ventilation?
Lung Volumes • Tidal volume (TV) • Inspiratory reserve volume (IRV) • Expiratory reserve volume (ERV) • Residual volume (RV)
Lung Capacities • Vital capacity • Inspiratory capacity • Functional residual capacity • Total lung capacity
Dynamic Lung Function • Maximum voluntary ventilation • Forced vital capacity (FVC) • Forced expiratory volume (FEV) • FEV1.0 • Minute volume
Question Which measure of lung function indicates the total amount of air that the lungs can hold? • Tidal volume • Functional residual capacity • Vital capacity • Total lung capacity
Answer D. Total lung capacity Ratioanale: Total lung capacity (TLC) is the maximum amount of air that the lungs can hold—everything (volume-wise) at the end of a maximal inhalation (the deepest breath one can possibly take). Normal TLC is approximately 6 L.
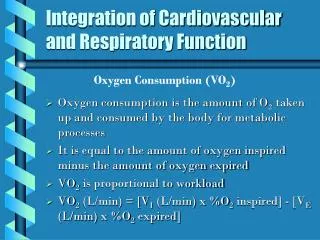
Gas Exchange • Oxygen moves from alveolar air into blood. • Carbon dioxide moves from blood into alveolar air.
Ventilation and Perfusion Scenario: An inhaled peanut blocks a left primary bronchus. Questions: • How will the ventilation in the two lungs change? • How will the composition of the air in the two lungs differ? • Which lung should receive more blood? • How should the body alter perfusion of the lungs?
Ventilation-Perfusion Mismatching • Blood goes to parts of the lung that do not have oxygen to give it. • Blood does not go to parts of the lung that have oxygen.
Question True or false? Ventilation-perfusion mismatch results in hypoxia.
Answer True Rationale: In either case (ventilation without perfusion or perfusion without ventilation), oxygen is not picked up by the capillaries and delivered to the tissues. The result of decreased oxygen at the tissue level is termed hypoxia.
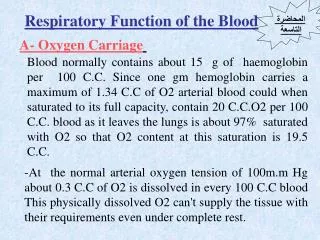
Blood Gases—Oxygen • Dissolved oxygen = PaO2 orPO2 • Normal value greater than 80 mm Hg • Oxygen bound to hemoglobin = oxyhemoglobin • Normal value 95% to 97% saturation
Hemoglobin Holds Four Oxygen Molecules • How saturated is this molecule of hemoglobin? • How could a person have a hemoglobin saturation of 95%?
Oxygen Capacity • Amount of oxygen the blood can hold. • What is the oxygen capacity of normal blood? • What is the oxygen capacity of anemic blood?
Oxygen Release • If the blood released half of its oxygen to the tissues: • How much oxygen would the normal tissues receive? • How much would the anemic person's tissues receive?
Oxygen Release (cont.) • Most body tissues have a PO2 of 40 to 60 mm Hg. • How much oxygen does the normal blood release at a PO2 of 40 mm Hg? • The anemic blood?
Blood Gases—Carbon Dioxide • Dissolved carbon dioxide = PaCO2 orPCO2 • Normal value 35 to 45 mm Hg • Carbon dioxide bound to hemoglobin = carbaminohemoglobin • Carbonic acid bicarbonate ion and H+ • When you exhale, you remove CO2 from your blood and also decrease the amount of carbonic acid, raising your blood pH.
Question True or false? The relationship between PCO2 and pH is direct.
Answer False Rationale: The relationship is indirect. As PCO2 levels rise, the amount of carbonic acid in the blood increases, making the pH more acidic (decreasing it).
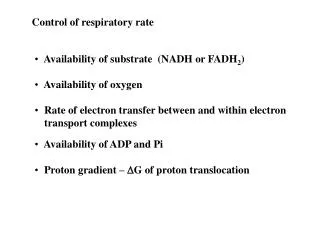
Chemoreceptors Can Adjust Respiration Rate • Central chemoreceptors • Measure PCO2 and pH in cerebrospinal fluid • Increase respiration when PCO2 increases or pH decreases • Peripheral chemoreceptors • Measure PO2 in arterial blood • Increase respiration when PO2 less than 60 mm Hg
Scenario You are caring for a COPD client. • He has chronically high PCO2. • He is being given low-flow oxygen and complains all the time that he “needs more air,” so you turn up his oxygen. Question: • When you check on him later, he is unconscious and not breathing. What happened?
Chapter 22Respiratory Tract Infections, Neoplasms, and Childhood Disorders
Upper Respiratory Viruses in Adults • Common cold • Rhinosinusitis • Influenza
The Common Cold • Rhinoviruses • Occur in early fall and late spring in persons between ages 5 and 40 • Parainfluenza viruses • Occur in children younger than 3 • Respiratory syncytial virus • Occur in winter and spring in children younger than 3 • Coronaviruses and adenoviruses • Occur in winter and spring
Rhinosinusitis (Sinusitis) • Infection or allergy obstructs sinus drainage • Acute: facial pain, headache, purulent nasal discharge, decreased sense of smell, fever • Chronic: nasal obstruction, fullness in the ears, postnasal drip, hoarseness, chronic cough, loss of taste and smell, unpleasant breath, headache
Influenza • In the United States, approximately 36,000 persons die each year of influenza-related illness. • Transmission is by aerosol (three or more particles) or direct contact. • Upper respiratory infection (rhinotracheitis): • Like a common cold with profound malaise • Viral pneumonia: • Fever, tachypnea, tachycardia, cyanosis, hypotension • Respiratory viral infection followed by a bacterial infection.
Question For which viruses is a 2-year-old most at risk? • Rhinoviruses • Parainfluenza viruses • Respiratory syncytial virus (RSV) • All of the above • A and B
Answer E. A and B Rationale: Slightly older children (≥5 years of age) are at risk for rhinoviral infections. Children under the age of 3 are at risk of infection from both parainfluenza viruses and RSV.
Pneumonia—Inflammation of Alveoli and Bronchioles • Typical: bacteria in the alveoli • Lobar: affects an entire lobe of the lung • Bronchopneumonia: patchy distribution over more than one lobe • Atypical • Viral and mycoplasma infections of the alveolar septum or interstitium
Tuberculosis • World’s foremost cause of death from a single infectious agent • Causes 26% of avoidable deaths in developing countries • Drug-resistant forms • Mycobacterium tuberculosis hominis • Aerobic • Protective waxy capsule • Can stay alive in “suspended animation” for years
Initial TB Infection • Macrophages begin a cell-mediated immune response • Takes 3 to 6 weeks to develop positive TB test • Results in a granulomatous lesion or Ghon focus containing • Macrophages • T cells • Inactive TB bacteria
Ghon Complex • Nodules in lung tissue and lymph nodes. • Caseous necrosis inside nodules. • Calcium may deposit in the fatty area of necrosis. • Visible on x-rays.