Respiratory function tests
Explore the fundamentals of respiratory function tests, including lung anatomy, lung volumes, and the mechanics of breathing. Discover the goals of respiration, lung capacities, and clinical significance. Learn about peak expiratory flow rate, spirometry, and factors affecting lung volume. Find out why respiratory function tests are essential for detecting diseases, evaluating treatments, and monitoring lung health. Discover how these tests help in assessing lung function and guiding medical interventions.

Respiratory function tests
E N D
Presentation Transcript
Respiratory function tests Prepared by: Dr. Ola S. Ziara
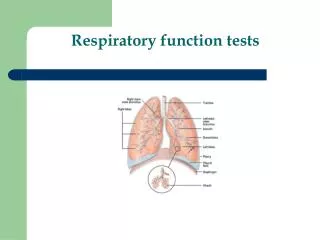
Lung anatomy and physiology • Lungs consist of • Airways • Alveoli
Airways • Conducting zone: no gas exchange occurs • Anatomic dead space • Transitional zone: alveoli appear, but are not great in number • Respiratory zone: contain the alveolar sacs
Mechanics of Breathing • Inspiration • Active process • Expiration • Quiet breathing: passive • Can become active , with forced expiration
The goals of respiration: • Provide O2 to tissue and remove Co2 through: • Pulmonary ventilation: outflow and inflow of air between outside and alveoli. • Diffusion of O2 and Co2 between alveoli and blood. • Transport to and from tissue
Lung Volumes IRV IC VC TLC TV ERV FRC RV RV
Tidal Volume (TV) • Volume of air inspired or expired during normal quiet breathing • About 500ml IRV IC VC TLC TV ERV FRC RV RV
The extra volume of air that can be inspired over and above the normal tidal volume , when person inspires with full force =3000ml The Inspiratory Reserve Volume IRV IRV IC VC TLC TV ERV FRC RV RV
The extra volume of air that can be exhaled over normal tidal volume when person expires forcefully ERV= 1100ml Expiratory Reserve Volume (ERV) IRV IC VC TLC TV ERV FRC RV RV
Volume of air remaining in the lungs at the end of maximum expiration. RV =1200 ml Residual Volume (RV) IRV IC VC TLC TV ERV FRC RV RV
Vital Capacity (VC) • The maximum amount of air a person can expel from the lungs after filling the lungs to their maximum extent and then expires to the maximum extent. • VC=4600ml • VC=IRV+TV+ERV IRV IC VC TLC TV ERV FRC RV RV
Inspiratory Capacity (IC) • The amount of air a person can breathe in beginning at the normal expiratory level and distending the lung to the maximum amount. • IC = IRV + TV • IC= 3500ml IRV IC VC TLC TV ERV FRC RV RV
Functional Residual Capacity (FRC) • Volume of air remaining in the lungs at the end of a normal expiration • FRC = ERV + RV • FRC= 2300 ml IRV IC VC TLC TV ERV FRC RV RV
Total Lung Capacity (TLC) • Volume of air in the lungs after a maximum inspiration • TLC = IRV + TV + ERV + RV • =5800ml IRV IC VC TLC TV ERV FRC RV RV
CLINICAL SIGNIFICANCE • VC depends on sex, age and height. • VC < 80% is abnormal. • As in cases of restrictive ventilation disorder • RV/TLC% (residual air rate) normal : < 35% emphysema: > 40 % old person can be 50%. • FRC ↑ : emphysema • FRC ↓ : interstitial pulmonary fibrosis
Value of Respiratory function tests • Evaluates 1 or more major aspects of the respiratory system • Lung volumes • Airway function • Gas exchange
Why to use Respiratory function test? • Detect disease • Evaluate extent and monitor course of disease • Evaluate treatment • Assess risk for surgical procedures
Investigation tools used for studying respiratory function • Arterial blood gases • Blood PH • Pulse oximeter • Peak flow meter measuring peaked expiratory flow rate. • Spirometry
Factors affecting lung volume • Age • Sex • Height • Weight • Race • Disease
Peak flow meter is a small device that measures the fastest rate of air that you can blow out of your lungs, it can detect airway narrowing, commonly used in asthma, Even by the patient himself to know • when he needs an emergency interference. • the effectiveness of a person's asthma management and treatment plan. • when to stop or add medication, as directed by physician. • what triggers the asthma attack (such as exercise-induced asthma )
PEAKED EXPIRATORY FLOW • To perform this test: • Loosen any tight clothing that might restrict your breathing. • Sit up straight or stand while performing the tests • Breathe in as deeply as possible. • Mouthpiece is placed in mouth with lip sealed to prevent escape of air • Blow into the instrument's mouthpiece as hard and fast as possible. • Do this three times, and record the highest flow rate. • Why the Test is Performed? • The test is commonly used to diagnose and monitor lung diseases such as: • Asthma • Chronic obstructive pulmonary disease (Less accurate)
Normal Results • Normal values vary based on a person's age, sex, and size. Peak flow measurements are most useful when a person compares the number on a given day to his or her "personal best." • A fall in peak flow can signal the onset of a lung disease flare, especially when it occurs with symptoms such as: Shortness of breath Increased cough Wheezing
SPIROMETRY • Simple, office-based • Measures flow, volumes • Volume vs. Time • Can determine: - Forced expiratory volume in one second (FEV1) - Forced vital capacity (FVC) - FEV1/FVC
Indications of spirometry:diagnostic and prognostic • Evaluation of signs and symptoms of pulmonary diseases like asthma and COPD • Screening at-risk populations (male smokers >45 years) • Monitoring pulmonary drug toxicity • Preoperative assessment • Assess severity of diseases • Follow up response to therapy • Determine further treatment goals • Referral for surgery • Disability
Terminology • Forced vital capacity (FVC): • Total volume of air that can be exhaled forcefully from TLC • The majority of FVC can be exhaled in <3 seconds in normal people, but often is much more prolonged in obstructive diseases • Measured in liters (L)
FVC • Interpretation of % predicted: • 80-120% Normal • 70-79% Mild reduction • 50%-69% Moderate reduction • <50% Severe reduction
FEV1 • Forced expiratory volume in 1 second: (FEV1) • Volume of air forcefully expired from full inflation (TLC) in the first second • Measured in liters (L) • Normal people can exhale more than 75-80% of their FVC in the first second; thus the FEV1/FVC can be utilized to characterize lung disease
FEV1 • Interpretation of % predicted: • >75% Normal • 60%-75% Mild obstruction • 50-59% Moderate obstruction • <49% Severe obstruction
Technique • Have patient seated comfortably • Closed-circuit technique • Place nose clip on • Have patient breathe on mouthpiece • Have patient take a deep breath • Blow out the air as fast as possible and as hard and long as possible
Obstructive Lung Disease — DifferentialDiagnosis • Asthma • COPD - chronic bronchitis • Bronchiectasis • Bronchiolitis • Upper airway obstruction
Restrictive lung disease: • Pneumoconiosis • Chest wall deformity • Pleural adhesion and pleural effusion • Interstitial lung fibrosis • Combined restrictive and obstructive in cases of cystic fibrosis
Flow-Volume Loop • Illustrates maximum expiratory and inspiratory flow-volume curves • Useful to help characterize disease states (e.g. obstructive vs. restrictive)
Obstructive Disorders • Characterized by a limitation of expiratory airflow • Decreased: FEV1, FEV1/FVC ratio (<0.8) • Increased or Normal: TLC
Spirometry in Obstructive Disease • Slow rise in upstroke • May not reach plateau
Restrictive Lung Disease • Characterized by diminished lung volume • Decreased TLC, FVC • Normal FEV1 • Normal or increased: FEV1/FVC ratio
Restrictive Disease • Rapid upstroke as in normal spirometry • Plateau volume is low
Bronchial Dilation Test • Method: to determine FEV1 and FEV1/FVC% before and after ß2-agonist inhalation • Result: improved rate = after-before ×100% before Positive: >15% • Reversible limitation: asthma
Emphysema • Loss of alveolar structure by increased proteolytic breakdown, destruction of elastic tissue in alveolar walls • Decreased Expiratory flows • Increased air trapping, RV/TLC • Decreased capillary surface area for gas exchange • No Response to BD challenge