Download

1 / 23
230 likes | 334 Vues
Joan Blackwood Clinical Lead MH Service Re-design Frances Paton Business Intelligence Manager (Partnerships) Fiona McMahon Senior Practitioner, Re-admissions/Service Improvement. “Improving Care Delivery and the Patient Experience”. The A&E and Mental Health Pathway.

E N D
Joan Blackwood Clinical Lead MH Service Re-design Frances Paton Business Intelligence Manager (Partnerships) Fiona McMahon Senior Practitioner, Re-admissions/Service Improvement
“Improving Care Delivery and the Patient Experience” The A&E and Mental Health Pathway
2010/2011 GG&C Performance and Development Plan – Contribution to Acute Services Framework (HEAT 10) GG&C A&E Attendances Steering Group GG&C MH and A&E Acute Interface Working Group (Lead - Calum MacLeod Head of Mental Health South Glasgow) Background
Multi disciplinary and management representation from A&E, Mental Health, Addictions, A&E Attendances Group, Homelessness, Liaison, Information Services etc. 4 hour breaches + reasons Repeat attendances Clinical Pathways Clinical Sub Group MH and A&E Acute Interface Working Group
Information Areas that need to be explored - those with common causes for delay • Wait for 1st Assessment • Wait for Specialist Assessment • Wait for Psychiatric Bed • Wait for Transport
Greater Glasgow & Clyde – Phase 1 • Identify patients who are A&E Breachers • Identify all A&E attendances who have a MH diagnosis and are known to our services. To do this we - • Extracted all Mental Health A&E presentations. (North & South A&E – not Clyde) • Extracted all MH data recorded on PIMS (Inpatient, CMHT, Crisis etc). • Merged into one database to identify patients. (Patient Linkage) • Resulted in ‘draft’ suite of information reports linking in with Service use .
Snapshot of Information Reports (Period: 01/10/2009 – 31/03/2010) Last known MH Service prior to A&E presentation Presentations where A&E Diagnosis is Categorised 7,057 MH presentations, CHI present in 6,296 (4,864 patients) so Reports are based on these 6,296 records • Better use of information to help inform decision making.
Snapshot of Information Reports Associated CMHT’s for Patient • Better use of information to help inform decision making.
CLINICAL PORTAL • What is Clinical Portal? • A web-based system that presents all electronic information for a patient in a single location • The Portal uses technology to provide a clinician-friendly view of information from multiple information sources. • Mental Health data on Clinical Portal • Data items to be published in the Mental Health clinical Portal are: • Alerts • Open Referrals • Diagnoses • Last Contact • Last Clinic Attendance • Mental Health Sparra on Clinical Portal • Predictive algorithm, developed by ISD. It identifies patients aged 15 years and over at risk of re-admission to a psychiatric hospital or unit.
Next Steps • ‘Work in Progress’ • Consolidate and agree information requirements between services • The initial information analysis has prompted questions about Clinical Pathways between A&E and Mental Health including Addictions
As a result of the data collection exercise reports can now be made available to highlight : Patients who are known to both A&E and Mental Health Services Are regular attendees at A&E Regularly breach the 4 hour target Mental Health, A&E & Addictions Patient Pathway
We needed to gain a better understanding of the patient journey. To identify gaps, blocks, delays, demand and capacity issues across services. Most importantly we wanted to know what was happening to patients. But
Sub-Group established included clinical staff from : A&E, Adult Community Mental Health, Crisis (day & night OOH) Liaison Psychiatry, Inpatients and Addictions Remit of Group: To carry out a process mapping exercise to accurately inform routes into and out of A&E To test clinical scenarios across the process map and identify current systems To support effective interface across all services Mental Health, A&E & Addictions Patient Pathway
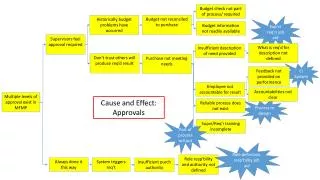
Three meetings – task and finish approach Plan – scope and range of the work Process map – involving all stake holders Follow up issues identified and action plan developed Process
Feedback Progress – MH and A&E Acute Interface Working Group, GG&C Attendances Group Four dimensions to the action plan – Clinical Practice Information Service Response Patient Experience Extend membership of Clinical Group to reflect the further work required on pathways Next Steps
Information – Using information to help inform and improve clinical practice. Clinical Portal – A&E Staff will have access to Mental Health Service Data. Clinical Response – What is the expected response by A&E and Mental Health Staff. Develop Clinical Practice Guidelines – to access management/crisis plans, develop case review mechanisms. Service response – further work to be done with other parts of the Mental Health Service i.e. Addictions Action Plan – “A Taster”