Download
1 / 43
430 likes | 681 Vues
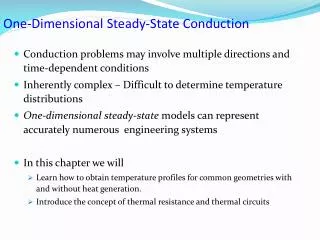
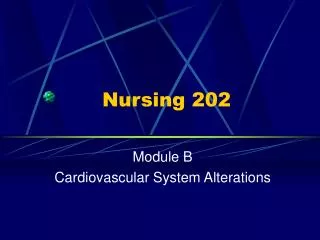
Basic physiologic properties of myocardium: automaticity conduction excitability (refractoriness) contractility. M ( 1 ). Aorta. SA uzel. VCI. Sval síní. AV uzel. 1. Subend. přední ram. SA uzel. Spol. svazek. Internodální spoje. Raménko. AV uzel. Purk. vlákna. Sval komor.

E N D
Basic physiologic properties of myocardium: automaticity conduction excitability (refractoriness) contractility
M (1) Aorta SA uzel VCI Sval síní AV uzel 1 Subend. přední ram. SA uzel Spol. svazek Internodální spoje Raménko AV uzel Purk. vlákna Sval komor Hisův svazek Pravé raménko ECG T P U QRS Purkyňova vlákna 0.4 0.6 0.2 Subendokardiální zadní raménko Čas (s)
Effective refractory period The period that must pass after the upstroke of a conducted impulse in a part of the heart before a new action potential can be propagated in that cell or tissue.
Arrhythmias are defined by exclusion- i.e., any rhythm that is not a normal sinus rhythm (NSR) is an arrhythmia. Abnormal automaticity Sick sinus syndrome Pacemaker activity that originates anywhere other than in the sinoatrial node = abnormal autom. Abnormal conduction Conduction of an impulse that does not follow the physiological path (defined previously) reenters tissue previously excited = reentry
Supraventricular tachycardia A reentrant a arrhythmia that travels through the AV node; it may also be conducted through atrial and ventricular tissue as part of the reentrant circuit Ventricular tachycardia A very common arrhythmia, associated often with myocardial infarction; ventricular tachycardia (a) may involve abnormal automaticity or abnormal conduction, (b) usually impairs cardiac output, and (c) may deteriorate into ventricular fibrillation; requires prompt management
Atrial, ventricular fibrillation Arrhythmias involving rapid reentry and chaotic movement of impulses through the tissue of the atria or ventricles; ventricular, but not atrial, fibrillation is fatal within a few minutes if not terminated
A few of the clinically important arrhythmias are: atrial flutter, atrial fibrillation (AF), atrioventricular nodal reentry (a common type of [SVT]), premature ventricular beats (PVBs), ventricular tachycardia (VT), ventricular fibrilation (VF).
Drug class Classifications: The antiarrhythmic agents are often classified using a system loosely based on the channel or receptor involved. This system specifies four classes, usually denoted by Roman numerals I through IV: I. Sodium channel blockers II. Beta adrenoceptor blockers III. Potassium channel blockers IV. Calcium channel blockers A miscellaneous class includes adenosine, digitalis, potassium iod, and magnesium ion.
Class I - sodium channel blocking drugs all of them behave like local anesthetics. These agents are frequently subdivided according to their effects on action potential duration and upstroke velocity (Vmax): Prototypes: Class IA agents (prototype, quinidine) prolong the action potential and reduce Vmax (++). Class IB drugs shorten the action potential in some cardiac tissues (prototype, lidocaine) and Vmax (±). Class IC drugs have no effect on action potential duration (prototype, flecainide) but Vmax.
Mechanism of action: all class I drugs slow or abolish abnormal pacemakers and slow or block conduction (especially in depolarized cells) wherever these processes depend on sodium channels Useful sodium (and calcium) channel-blocking drugs bind to their receptors much more readily when the channel is open or inactivated than when it is fully repolarized and recovered from its previous activity. Ion channels in arrhythmic tissue spend more time in the open or inactivated states than do channels in normal tissue. Therefore, these antiarrhytmic drugs block channels in abnormal tissue more effectively than channels in normal tissue.
As a result, antiarrhythmic sodium (and calcium) channel blockers are statedependent in their action, ie, selectively depressants on tissue that is frequently depolarizing (eg, during a fast tachycardia) or is relatively depolarized during rest (by hypoxia). Drugs with classIA action: Quinidine is the class IA prototype. procainamide, disopyramide and amiodarone
Quinidine C a r d i a c effects: direct (concentration dependent) A-V depressant negative inotropic concentration independent parasympatolytic increase action potential (AP) duration and the effective QT interval. E x t r a c a r d i a c effects: quinidine possesses alpha adrenoceptor-blocking properties that can cause vasodilation and a reflex increase in sinoatrial nodal rate.
Pharmacokinetics Quinidine is usually administered orally and is rapidly absorbed from the gastrointestinal tract. It is 80% bound to plasma proteins. Its half-life is about 6 hours and may be longer in patients with congestive cardiac failure or hepatic or renal disease. Is is usually administered as the sulfate, gluconate, or polygalacturonate salt. The usual dose of 0.2-0.6 g of quinidine sulfate is given 2-4times daily. Parenteral administration of quinidine is occasionally necessary. Quinidine is absorbed after i.m. injection of the sulfate in oil or the aqueous gluconate preparation. IV administration is usually associated with a decline in blood pressure as a result of its peripheral vasodilating action.
Toxicity: Quinidine has antimuscarinic actions in the heart that inhibit vagal effects. This can overcome some of its direct membrane effect and lead to increased sinus rate and increased atrioventricular conduction. This action can be prevented by prior administration of a drug that slows atrioventricular conduction (verapamil, a beta-blocker, digitalis). A small percentage (1-5%) of patients given quinidine develop a syndrom called "quinidine syncope" characterized by recurrent light-headedness and episodes of fainting. torsade de pointes
These toxic effects are more likely to occur when the serum concentrations exceed 5 ug/ml and in the presence of high serum potassium levels (> 5mmol/l) Widening of the QRS duration by 30% by quinidine administration is usually considered premonitory of serious toxicity. Toxic concentrations may depress contractility and lower blood pressure. Quinidine causes cinchonism (headache, tinnitus); cardiac depression; gastrointestinal upset; and allergic reactions (eg, thrombocytopenic purpura). Quinidine reduces the clearance of digoxin and may increase the serum concentration of the glycoside to dangerous levels.
Therapeutic use: Quinidine is used in nearly every form of arrhythmia: premature atrial contractions, paroxysmal atrial fibrillation and flutter, intra-atrial and atrioventricular nodal reentrant arrhythmias, premature ventricular contractions, and ventricular tachycardias. especially chronic outpatient treatment.
Procainamide The electrophysiological effects of procainamide are similar to those of quinidine. Procainamine ´s cardiotoxic effects are similar to those of quinidine. The most troublesome adverse effect is a syndrome resembling lupus erythematosus and usually consisting of arthralgia and arthritis. Approximately one-third of patients receiving long-term procainamide therapy develop this syndrome.
Pharmacokinetics: Procainamide can be administered safely IV, i.m. and is well absorbed orally. The major metabolite is N-acetylprocainamide (NAPA) - pharmacologically active. Excessive accumulation of NAPA has been implicated in torsade de pointes during procainamide therapy. Some individuals rapidly acetylate procainamide and develop high level of N-acetylprocainamide. The lupus syndrom appears to be less common in these patients.
One arrhythmia, called torsade de pointes, is particularly associated with quinidine and other drugs that prolong AP duration (except amiodarone). Hyperkalemia usually exacerbates the cardiac toxicity of class I drugs. Treatment of overdose with these agents is usually carried out with sodium lactate (to reverse drug-induced arrhythmias) and pressor sympathomimetics (to reverse drug-induced hypotension).
Drugs with class IB actions: Lidocaine is the prototype IB drug. This drug affects ischemic or depolarized Purkinje and ventricular tissue and has little effect on atrial tissue; the drug reduces action potential duration, but because it slows recovery of sodium channels from inactivation, it does not shorten (or may even prolong) the effective refractory period. Mexiletine, tocainide and fenytoin have similar effects. Because these agents have little effects on normal cardiac cells, they have little effects on the ECG..
Lidocaine is useful in acute ventricular arrhythmias, especially those involving ischemia, eg, following myocardial infarction. Atrial arrhythmias are not respondsive unless caused by digitalis. Lidocaine is usually given intravenously, but IM administration is also possible. Mexiletine and tocainide have similar actions but can be given orally. Typical local anesthetic toxicityCNS stimulation, including convulsions; cardiovascular depression (usually minor); allergy (usually rashes but may extend to anaphylaxis). Tocainide may cause agranulocytosis. These drugs may also precipitate arrhythmias, but this is less common than with class IA drugs. Hyperkalemia, however, increases cardiac toxicity.
Drugs with class IC action: Flecainide is the prototype drug with class IC actions. Encainide (recently withdrawn), moricizine, and propafenone These drugs have no effect on ventricular action potential duration or the QT interval. They are powerful depressants of sodium current, however, and can markedly slow conduction velocity in atrial and ventricular cells
Flecainide is effective in both atrial and ventricular arrhythmias, but is approved only for (a)refractory ventricular tachycardias that tend to progress to VF at unpredictable times, resulting in "sudden death", and (b) certain intractable supraventricular arrhythmias. more likely than other antiarrhythmic drugs to exacerbate or precipitate arrhythmias (proarrhythmic effect). For this reason, the class IC drugs are limited to last report applications in refractory tachycardias. These drugs also cause local anesthetic-like CNS toxicity. Hyperkalemia increases the cardiac toxicity of these agents.
CLASS II (BETA-BLOCKERS) Propranolol and esmolol are the prototype antiarrhythmic beta-blockers. Their mechanism in arrhythmias is primarily cardiac beta blockade and reduction in cAMP, which results in the reduction of both sodium and calcium currents and the suppression of abnormal pacemakers. The AV node is particularly sensitive to beta-blockers; the PR interval is frequently prolonged by class II drugs (Table 14-2). Under some conditions, they may have some direct local anesthetic (membrane stabilizing) effect in the heart, but this is probably rare at the concentrations achieved clinically.
Esmolol a very short-acting beta-blocker for intravenous administration, is used almost exclusively in acute surgical arrhythmias. Propranolol, metoprolol, and timolol are commonly used as prophylactic drugs in patients who have has a myocardial infarction. These drugs provide a protective effect for two years or more after the infarct. The toxicities of beta-blockers are the same when used as antiarrhythmics or in any other application. However, patients with arrhythmias are often more prone to b-blocker-induced depression of cardiac output than are patients with normal hearts.
CLASS III (POTASSIUM CHANNEL BLOCKERS) Sotalol is a chiral compound, ie, it has two optical isomers. One isomer is an effective beta-blocker, the other provides most of the antiarrhythmic action. The clinical preparation contains both isomers. Bretylium is an older drug that combines sympathoplegic actions and a potassium channel-blocking effect.
Amiodarone most efficacious antiarrhythmic drug. broad spectrum: it blocks sodium, calcium, and potassium channels and beta adrenoceptors. Toxicity thyroid dysfunction (hyper- or hypothyroidism), paresthesias, tremor, microcrystalline deposits in the cornea and skin, and pulmonary fibrosis. Amiodarone rarely causes new arrhythmias.
Mechanism & effects prolongation of the action potential duration is cause by blockade of potassium channels that are responsible for the repolarization of the action potential. AP prolongation results in an increase in effective refractory period and reduces the ability of the heart to respond to rapid tachycardias. Sotalol and amiodarone (and quinidine) produce this effect on most cardiac cells; the action of these drugs is therefore apparent in the ECG. N-acetylprocainamide (NAPA), a metabolite of procainamide, also significatnly prolongs the action potential and the QT interval. Bretylium, on the other hand, produces AP prolongation mainly in ischemic cells, and causes little change in the ECG.
C. Clinical uses & toxicities: Bretylium is used only in the treatment of refractory postmaocardial infarction arrhythmias, eg, recurrent ventricular fibrillation. The drug is rarely used. It may precipitate new arrhythmias or marked hypotension. Sotalol is more generally useful and is available by the oral route (Table 14-2). Sotalol may precipitate torsade de pointes arrhythmia, as well as signs of excessive beta blockade such as sinus bradycardia or asthma. The toxicities of amiodarone and other class IA drugs (which share the potassium channel-blocking action of class III agents) are discussed with the class IA drugs.
CLASS IV (CALCIUM CHANNEL BLOCKERS) A. Prototype: Verapamil is the prototype. Diltiazem is also an effective antiarrhythmic drug although it is not approved for this purpose. Nifedipine and the other dihydropyridines are not useful as antiarrhythmics, probably because they decrease arterial pressure sufficiently to evoke a compensatory sympathetic discharge to the heart. The latter effect would facilitate rather than suppress arrhythmias.
B. Mechanism & effects: Verapamil and diltiazem are effective in arrhythmias that must traverse calcium-dependent cardiact tissue (eg, the atrioventricular node). These agents cause a state-dependent selective depression of calcium current in tissues that require the participation of L-type calcium channels (Figure 14-7). Conduction velocity is decreased and effective refractory period is increased by these drugs. PR interval is consistently increased (Table 14-2).
C. Clinical use & toxicities: Calcium channel blockers were drugs of choice in atrioventricular nodal reentry (also known as nodal tachycardia and supraventricular tachycardia) until adenosine became available; they are highly effective in this type of arrhythmia. Their major use now is in the prevention of these nodal arrhythmias. These drugs are orally active; verapamil is also availabel for parenteral use (Table 14-2). The most important toxicity of verapamil as an antiarrhythmic relates to excessive pharmacologic effect, since cardiac contractility can be significantly depressed. See chapter 12 for additional discussion of toxicity. Amiodarone has moderate calcium channel- blocking activity.
MISCELLANEOUS ANTIARRHYTHMIC DRUGS A. Adenosine: Adenosine is a normal component of the body, but when given in high dosage (6-12 mg) as an intravenous bolus, the drug markedly slows conduction in the atrioventricular node (Table 14-2). Adenosine is extremely effective in abolishing AV nodal arrhythmias and, because of its very low toxicity, has become the drug of choice for this arrhythmia. Adenosine has an extremely short duration of action these effects do not limit the use of the drug.
B. Digitalis: The actions of digitalis were discussed in Chapter 13. The cardiac parasymathomimetic action of digoxin is sometimes exploited in the treatment of rapid atrial or AV nodal arrhythmias. In atrial flutter or fibrillation, digitalis slows AV conduction sufficiently to protect the ventricles from excessively high rates. In AV nodal reentrant arrhythmias, digitalis may exert enough depressant effect to abolish the arrhythmia. The latter appliaction of digitalis has become less common since the development of calcium channel blockers and adenosine as antiarrhythmic drugs.
C. Potassium ion: Potassium depresse ectopic pacemakers, including those caused by digitalis toxicity. Hypokalemia is associated with increased incidence of arrhythmias, especially in patients receiving digitalis. Conversely, excessive potassium levels depress conduction and can measured and, if abnormal, normalized. D. Magnesium ion: Magnesium has not been as well studied as potassium but appears to have similar depressant effects on digitalis-induced arrhythmias. Magnesium also appears to be effective in some cases of torsade de pointes arrhythmia.