Download
1 / 38
420 likes | 971 Vues
Medial Elbow Instability. Geoff Wilkin Academic Half-Day University of Ottawa, Div. of Orthopaedic Surgery April 19, 2012. Outline. Biomechanics of Throwing Medial Elbow Instability Valgus Extension Overload. Throwing Biomechanics. Throwing Biomechanics. Windup.

E N D
Medial Elbow Instability • Geoff Wilkin • Academic Half-Day • University of Ottawa, Div. of Orthopaedic Surgery • April 19, 2012
Outline • Biomechanics of Throwing • Medial Elbow Instability • Valgus Extension Overload
Windup • Weight to trailing leg, lead leg flexes • Trunk rotates away from target • Elbow flexed • Forearm pronated • Ends when ball leaves glove hand
Early Cocking • Stride initiation • Lead leg and hip drive toward target • Shoulder abduction and ER • Elbow extension controlled eccentrically • Ends when lead foot contacts ground
Late cocking • Shoulder abduction to 90° and ER to maximum (150-180°) • Elbow flexes to ~90° • Forearm pronates • Leading leg decelerates and pelvis rotates toward target • L-spine lordosis increases shoulder ER • Ends at max shoulder ER
Acceleration • Humerus rapidly transitions to IR, propelled by body rotation • Trunk flexes, elbow extends • Acceleration ~600,000 deg/sec2 • Max varus torque ~64 N⋅m • Ends with ball release
Deceleration/Follow-through • Nearly equally rapid deceleration (~500,00 deg/sec2) • Arm continues into horizontal adduction, shoulder IR, elbow extension • Posterior shoulder girdle muscles, cuff/deltoid, & elbow flexors decelerate arm • Weight transfer to lead leg
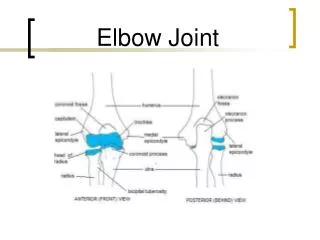
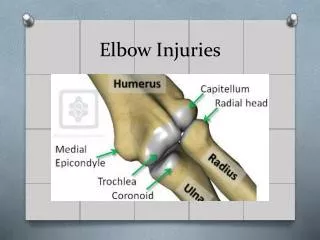
Anatomy • Medial Collateral Ligament • Anterior Bundle • Strongest (260 N) • Primary Valgus stabilizer • Posterior Bundle • Transverse Bundle
Anterior Bundle • Origin: anteroinferior medial epicondyle • slightly posterior to axis of rotation = cam effect • Anterior Band: 0-60/90 • Posterior Band: 60/90-120 • Insertion: • sublime tubercle • ~18mm distal to coronoid tip
Valgus Restraint of MCL • Morrey & An, AJSM 1983 • 31% at 0° • 54% at 90° (less bony stability) • Morrey et al., CORR 1991 • Sequential removal: radial head, PMCL, AMCL • MCL is primary valgus stabilizer • Radial head important secondary stabilizer when MCL deficient
Muscles • Flexor-pronator mass • Dynamic secondary stabilizers to valgus stress • Protect UCL • FCU may be most important due to synergistic position Davidson et al., AJSM 1995
Muscle • Small moment arm • Mechanical disadvantage • Limited ability to compensate for MCL deficiency • Hamilton et al., JSES 1996 • No compensatory increase in flexor/pronator activity in pitchers with MCL deficiency
Pathogenesis • Valgus overload in flexion • Acute rupture • valgus force exceeds yield strength of UCL • Repetitive microtrauma
Role of Throwing Mechanics • Aguinaldo & Chambers, AJSM 2007 • Increased elbow valgus loads with: • Early trunk rotation • Increased shoulder ER • Decreased elbow flexion • Sidearm delivery
Clinical Presentation • Medial-sided elbow pain • Insidious onset, occasionally acute • Late cocking & early acceleration phases • Weakness, loss of control & stamina towards end of game • +/- ulnar nerve symptoms
Physical Exam • ROM (may pitchers lack terminal extension) • Ulnar nerve • motor, sensory, subluxation, Tinel’s • Flexor-pronator strength
Physical Exam • Static Valgus Stress • pain at 70-90° • “Milking test”
Physical Exam • “Moving Valgus Stress test” • pain in mid-flexion (70-120°) • most accurate predictor of UCL injury • Sens: 100% • Spec: 75% O'Driscoll SWM et AL., Am J Sports Med. 2005 Feb.;33(2):231–239.
Imaging • Xray (AP, Lat, Obl) • Oblique axial at 110° • posteromedial osteophytes • valgus stress views • 0.5-2mm widening • utility is questionable (differences in technqiue, normal widening) • calcification of UCL
Imaging • MRI • Acute Injury • Sens: 57-79% • Spec: 100%
Management • Non-operative • Usually successful in non-throwing athletes • Rest, activity restriction • Graduated return to activities
Management • Acute Rupture • Richard et al, JBJS(A) 2008 • 11 athletes with acute UCL rupture • Direct repair through drill holes or with suture anchors • 11/11 had avulsion of UCL origin and superficial flexor-pronator muscles • 3/11 acute ulnar nerve palsies recovered by 6 months • 10/11 regained full ROM & returned to previous level of sport within 4-6 months
Management • Chronic Valgus Instability • UCL reconstruction • Palmaris longus, gracilis, EHL, allograft • Initially described by Jobe (1986) • Figure-8 through bone tunnels • Routine detachment of flexor-pronator tendon & ulnar n. transposition
Management • Variations • Docking technique • Interference screw
Outcomes • Jobe et al., JBJS(A) 1986 • 10/16 professional pitchers returned to same level of sport • 2/16 ulnar n. palsy, 3/16 ulnar n. paresthesias • Thompson et al., JSES 2001 • Flexor-pronator split, no ulnar n. transposition • 5% (4/83) ulnar n. symptoms • 82% “excellent” (return to same level >12 mo.), 12% “good” (return 1 level lower)
Rehab • 1 week - posterior splint • 1-3 weeks - hinged brace 10-110 • 3-4 weeks - full motion in brace • 4-6 weeks - sport specific activites • 12 weeks - gentle throwing with brace • 16 weeks - progress throwing out of brace
Etiology • Chronic UCL laxity • Impingement of the posteromedial tip of the olecranon on medial wall of olecranon fossa
History/Physical • Posterior or posteromedial elbow pain • Pain at ball release • late acceleration/deceleration vs. late cocking/early acceleration for UCL • Valgus stress in 20 and forced terminal extension • Tender posteromedial olecranon tip
Imaging • Posteromedial osteophytes • can be asymptomatic, & absence doesn’t exclude VEO • found in ~65% of professional baseball players undergoing sugery
DDx • Ulnar n. instability • anterior subluxation with flexion >90° • Olecranon stress fractures • symptoms during & after throwing. • pain more distal and lateral • Medial epicondylitis • tender epicondyle
Management • Initial Presentation • Active rest from throwing x 10-14 days • Recurrent Episodes • 4-6 weeks rest, more gradual return to throwing
Management • Operative • Arthroscopic debridement of posteromedial olecranon tip • How much? • Levin et al., JSES 2004 • 8mm
Prevention • Prevent overuse/overload of MCL • Good throwing mechanics • Pitch maximums • Minimize breaking pitches (sliders, curveballs, etc)