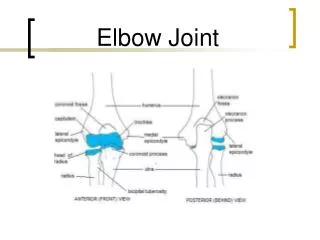
ELBOW
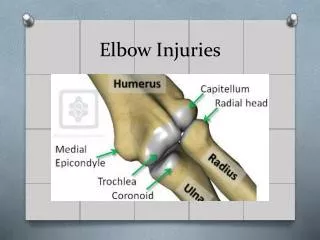
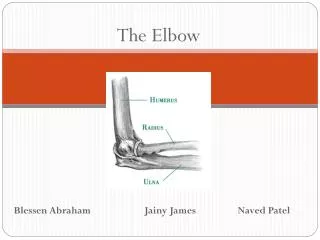
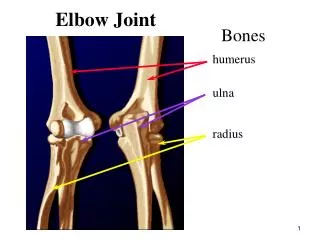
ELBOW. TRAUMATIC INJURIES OF THE ELBOW. Fractures distal end of the humerus Fractures proximal end of the radius Fractures proximal end of the ulna Dislocation of the elbow. Figure 7:Fracture distal end of the humerus. Management:

ELBOW
E N D
Presentation Transcript
TRAUMATIC INJURIES OF THE ELBOW • Fractures distal end of the humerus • Fractures proximal end of the radius • Fractures proximal end of the ulna • Dislocation of the elbow
Management: 1. Reduction and immobilizationin long arm cast or posterior slab with elbow flexion in case of posterior displacement and in elbow extension in case of anterior displacement for 2 to 3 weeks. 2. In complete displaced unstable fracture, K-wire fixation to maintain reduction(The pins are left in place for 4 to 6 weeks with elbow flexion). 3-Open reduction and internal fixationwith lag screws or medial and lateral reconstruction plates is used for intraarticular and extraarticular fracture when closed reduction failed.
Rehabiliatation: A)-Expected duration of rehabilitation: Twelve to 24 weeks. B) Range of motion: Within the first weeKof reduction and immobilization • Active range of motion of the fingers • Pendulum exercises for the shoulder, avoid internal and external rotation because it stresses the fracture site. • Gentle active elbow flexion and extension are allowed for stable fracture treated by open reduction internal fixation. • After one week, supervised elbow flexion from 90 degrees up with posterior splint immobilization between sessions
From 4 to 6 weeks: • Supervised active elbow range of motion is started for those using posterior slab. At 8 to 12 weeks: • Passive range of motion exercises to all joints of the extremity while focusing on flexion /extension of the elbow and pronation/supination of the forearm. The risk of myositis ossificans related to passive motion of the elbow hassignificantly decreased.
C)-Strength: Within the first week of reduction and immobilization • Isometric exercises for biceps, triceps and deltoid After the first week • Isometric exercises are added to forearm muscullature • No pronation /supination or shoulder external/internal rotation. • Begin grip strengthening exercises with ball or puttyAt eight to twelve weeks • Graduation of grip strength starting with weight of 1 to 2 pounds. • Progressive resistive exercises for elbow musculature: Begin with elbow flexion/extension. Weights (starting with 1 to 2 pounds and gradually increasing) are lifted against gravity.
D-Functional activities: • The patient is instructed to in using the uninvolved extremity for all functions of daily living. Clothes are donned on the involved first and doffed from the uninvolved extremity first. • From the 4th week, if rigid internal fixation was performed, the patient may use the involved extremity for eating and similar light activities. • At the 8th week, the involved extremity used for self-care and personal hygiene.
Complications: 1-Volkmann's ischemic contracture 2-Nerve injury: Commonly the median nerve 3-Myositis ossificans 4-Stiffness 5-Malunion 6-Ulnar nerve palsy
FRACTURES OF PROXIMAL END OF RADIUS Aetiology (mechanism of injury): Fractures of the radial head are usually caused by a fall onto the outstretched hand. Sign and symptoms Pain is felt around the lateral side of the elbow and is often aggravated by rotation of the forearm. Local swelling and tenderness over the radial head.
Rehabilitation: A-Expected duration: 6 to 12 weeks B- Range of motion: Within the first week: • Gentle active range of motion to elbow in flexion and pronation. • Active range of motion to the wrist and shoulder. From 4 to 6 weeks: • Continue with full active to active- assistive range of motion to the elbow in all planes • At the end of 6 weeks, if there is some limitation in the range of motion, gentle passive range of motion is allowed. • Only active and active-assistive range of motion for patient with internal fixation.
From 8 to 12 weeks: • Aggressive passive and active range of motion therapy should continue. There should be at least functional range of motion of the elbow. • Passive stretch motion may begin. • Hydrotherapy or fluidotherapycan be administered to facilitate range of motion. • Strength: • ball-squeezing exercises to the wrist and digits • At the second week, start gentle isometric exercises to the triceps, biceps, and deltoid. • At the 8th to 12th weeks: Start PRE to the elbow flexors, extensors, supinators, and pronators and to wrist flexors and extensors. Initially the patient can use the uninvolved extremity to offer resistance and thereby monitor his or her own tolerance.
D-Functional activities: • The uninvolved extremity is used for self-care and activities of daily living. • As the splint or sling is removed, the patient may don a shirt or blouse with the involved extremity first and doff it from the uninvolved extremity first. • At the 8th to 12th week, the involved extremity is used for self-care and light-duty activities. Heavy lifting or pushing with the involved extremity should be avoided.
FRACTURES OF PROXIMAL END OF THE ULNA Aetiology (mechanism of injury): Olecranon fractures are produced by direct blow to the point of the elbow, often by a fall. In direct injuries the fragments are often comminuted and there is more significant overlying soft tissue damage. Sign and symptoms There is pain around the elbow and usually swelling. The fracture gap can sometimes be felt. It is usually difficult or impossible for the patient to extend the elbow against resistance.
Figure 9: An olecranon fracture may be held together with a tension band fixation (illustration and X-ray).
Figure 10: A single medullary screw keeps the fractured bone together Plate and screws may be used to hold the broken bones in place.
Rehabilitation Goals The eventual goal of treatment for an olecranonfracture is to regain full motion of the elbow, as it was prior to the injury. Most patients will return to normal activities (except sports and heavy labor) within about 4 months, although full healing can take more than a year. Techniques After surgery, the patient's elbow may be splinted or casted for a short period of time. The patient may wear a sling if it provides comfort. Pain medications may be provided. The surgeon usually removes stitches or staples 10 to 14 days after surgery. The patient is often restricted from lifting objects with the injured arm for at least six weeks.
Motion exercises for the elbow and forearm should begin shortly after surgery, sometimes as early as the day after surgery. • Especially early after surgery, some patients may not be able to straighten their injured elbow on their own. To straighten the elbow, the patient needs to use his/her uninjured arm to help out, or assistance from another person. Full recovery from an olecranon fracture requires a lot of work. It is extremely important that exercises, once started, are performed multiple times a day, every day. The exercises only make a difference if they're done regularly. • Recovering strength often takes longer than expected; sometimes, 6 months ormore.
ELBOW DISLOCATION After the shoulder, the elbow is the second most frequently dislocated major joint. Types Posterior dislocations, in which the coronoid process disengages from the trochlea and moves posteriorly (Figure 11), account for more than 90% of dislocations .Whether the elbow dislocates posteromedially or posterolaterally, the injury and treatment are the same . Injured structures include the anterior and posterior bands of the medial collateral ligament and the lateral collateral ligament. The brachialis muscle, flexor-pronator muscle group, and articular cartilage may be injured as well.
Etiology: Fall on the outstretched hand . Signs 1-Obvious elbow deformity 2-Abnormal alignment of olecranon and both epicondyles: Management: • Reduction as soon as possible • Immobilize elbow in molded posterior plaster splint with elbow at 90 degrees flexion for 3 weeks • Gentle Range of motion after splinting • Never force range of motion (worsens injury)
Rehabilitation Program • Early ROM exercises in stable reduced elbow dislocations has been shown to be associated with an improved outcome. However, immobilization of the affected elbow for longer than 3 weeks in patients has been associated with loss of ROM compared with patients who start early ROM exercises. • Depending on the severity of the elbow dislocation, it may take several months for the elbow to fully heal. Muscle-strengthening activities, in addition to the ROM program, are important to improve endurance of the elbow. Incorporate sport-specific training as the athlete progresses through rehabilitation to ensure a safe return to his/her sport.
Complications: 1-Stiffness. 2-Late instability is not usually a problem, but posterolateral rotary instability, due to injury of the lateral ligaments, has recently been described . 3-Brachial artery disruption 4-Ulnar and Median nerve injury 5-Compartment syndrome may develop in the forearm fascia or biceps tendon due to massive swelling, which may occur in an acute elbow dislocation. Compartment syndrome must be considered in the differential diagnosis in the presence of persistent patient pain, particularly when exacerbations of pain occur with passive finger and wrist extension of the dislocated arm. 6-Ectopic calcification. 7-Myositis ossificans