Download
1 / 57
610 likes | 882 Vues
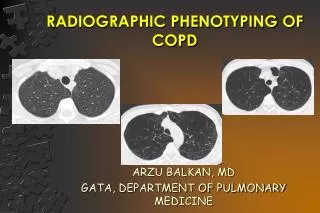
RADIOGRAPHIC PHENOTYPING OF COPD. ARZU BALKAN, MD GATA, DEPARTMENT OF PULMONARY MEDICINE. CONFLICT OF INTEREST DISCLOUSURE. There is no any conflict of interest in my presentation. OUTLINE. Basics of COPD radiology Measurement of emphysema Airway morphometry

E N D
RADIOGRAPHIC PHENOTYPING OF COPD ARZU BALKAN, MD GATA, DEPARTMENT OF PULMONARY MEDICINE
CONFLICT OF INTEREST DISCLOUSURE There is no any conflict of interest in my presentation.
OUTLINE • Basics of COPD radiology • Measurement of emphysema • Airway morphometry • Studies about radiographic phenotyping • Therapotic contribution of radiographic phenotyping
COPD • Small Airways Disease • Airway inflammation • Airway fibrosis, luminal plugs • Increased airway resistance • Parenchymal Destruction • Loss of alveolar attachments • Decrease of elastic recoil AIRFLOW LIMITATION
Changes in Small Airways in COPD Patients Inflammatory exudate in lumen Disrupted alveolar attachments Thickened wall with inflammatory cells - macrophages, CD8+ cells, fibroblasts Peribronchial fibrosis Lymphoid follicle Source: COLD 2007
Changes in Lung Parenchyma in COPD Alveolar wall destruction Loss of elasticity Destruction of pulmonary capillary bed ↑ Inflammatory cells macrophages, CD8+ lymphocytes Source: GOLD 2007
Chronic bronchitis Emphysema Airflow obstruction Asthma COPD Phenotyping • Emphysema sub-type • Emphysema distribution • Airways disease • Relative importance of components
Centrilobular emphsema Borders of holes have no perceptible wall
Panlobüler amfizem Sentrilobuler amfizem
Normal COPD
IMAGING TECHNICS • CHEST RADIOGRAPHY • THORAX CT • HIGH RESONANCE CT • MDCT • INSPIRATUAR-EKSPİRATUAR CT • SPİROMETRY (GATED) BT • MRG • 3 He MR
Measurement of Emphysema Qualitative assesment Quantitative assesment
Visual Scoring SEVERITY (%) 0 Yok 1 < 5 mm 2 > 5 mm 3 Difüz EXTENTION(% ) 1 % 1-25 2 % 26-50 3 % 51-75 4 % 76-100 • In general, visual inspection has yielded good correlations between CT and pathological measures of the extent and severity in all but the mildest cases • Visual assessment may lead to an overestimation of the extent of disease. • As an alternate to routine visual inspection: Minimum-intensity projection (MinIP) is more sensitive (%62- %81) • Spouge D, Mayo JR, Cardoso W, et al.J Comput Assist Tomogr 1993;17:710–713 • Gevenois PA, Yernault JC. Eur Respir J 1995;8:843–848 • emy-Jardin M, Remy J, Gosselin B, et al. Radiology 1996;200:665–671
Quantitative Assesment • Lung mask density. • Wall thickness. • Percentage of wall area. • Geometric measures: curvature of airway lumen.
Quantitative Assesment İntra / inter-observer variability is high Error ratio is high because of the oblique airways
Lung Mass Quantitative analysis 1-Definition of a lung mask is the first step of the processing pipeline. 2-Havayolları segmentlere ayrılır 3- Hava yollarının duvar kalınlıkları, havayolu duvar kalınlığının lümen genişliğine oranı • Airway Analysis • Lumen segmentation • Wall segmentation
LUNG MASK DENSİTY Mask extraction allows lung mask density analysis. Lung mask extraction for a HRCT
512 Pixels Pixel -550 -950 Voxel Principles of CT Densitometry
512 Pixels Pixel -550 -950 Voxel Principles of CT Densitometry
Airway measurement The softwares are devoloped automatic analysis of bronchial lumen and wall area on CT Focusing on the airway wall by traveling along the airway. New CT view in planes orthogonal to the airway.
Principles of Airway Morphometry Full Width Half Maximum
Ekspirium Lumen diameter/area Wall diameter/area Hipereiflation Mosaic perfusion Inspirium
CT acquisition technique and quantitative analysis of the lung parenchyma: variability and corrections • Bin Zheng*a, J. Ken Leadera, Harvey O. Coxsonb, Frank C. Scuirbac, Carl R. Fuhrmana, ArzuBalkand, Joel L. Weissfelde, Glenn S Maitza, David Gura • Proc of SPIE, 2006, 6143:2S-1 to 2S-8.
The Prevalence of Radiographic Emphysema in a Lung Cancer Screening Cohort • Balkan 1,2, F.C. Sciurba, MD2, C.R. Fuhrman2, S.N. Fisher2, D.O. Wilson2, J.G. Schragin2 ,J.L. Weissfeld2 1 GATA, Ankara, Turkiye 2 University of Pittsburgh, Pittsburgh, PA, USA Yayınlanmamış veri ATS 2005 , San Diego
Aim of the study • The purpose of the study is to explore the correlation between the degree of airflow obstruction as staged by GOLD criteria and the presence and severity of emphysema detected by low-dose helical CT scans in a large population of current and former smokers undergoing CT lung cancer screening.
Metod • 3301 participants • Low dose CT • Presence and absense of emphysema • Trace, mild, moderate, severeemphysema kategorilerineayrıldı • by using NETT multisentrikstudies’sstandartreferanceimages • The investigators developed a semiquantitative scoring system
Results In this study • There was no statistically difference according to genders, race and ethnicity.(p>0.05) • Results between the groups of age, smoking status, duration of cigarette use, dose and duration of smoking intensity, history, and GOLD were statistically different. (p<0.001p<0.001,<0.001,<0.001)
CT evidence of moderate emphysema was detected in 29 subjects with GOLD 0 spirometry..
Absence of CT evidence of emphysema was detected in 57 subjects with GOLD 3 or 4 spirometry
SFT’ye dayalı KOAH CT’ye dayalı KOAH Semptoma dayalı KOAH 1 %15.7
Conclusion • More studies are needed to standardize and validate CT that it did for spirometry in GOLD.
Conclusion • The ratio of CT detected emphysema is extremely high in smoker who has not been diagnosed with normal or airway obstructionn
Conclusion • Fizyolojik obstruksiyona karşı, herbir GOLD sınıflamasında sigaraya bağlı parankimal destrüksiyonun fenotipik görüntüsü arasında önemli farklılıklar mevcuttur.
Phenotyping of COPD patients according to CT emphysema score Boschetto P et al, Thorax 2006;61:1037
Phenotyping of COPD patients according to CT emphysema score Boschetto P et al, Thorax 2006;61:1037
Health related quality of life (SGRQ) varies by the extent of CT emphysema in severe COPD Martinez et al. AJRCCM 2007; 176: 243-52
CT phenotype and clinical correlates Han et al. COPD 2009; 6: 459-67
CT emphysema is associated with significant comorbidity • Lung cancer1,2,3 • Cardiovascular disease4,5,6 • Osteoporosis7,9 • Fat free mass loss9 1Wilson DO et al. AJRCCM. 2008; 178: 738-44; 2de Torres JP et al. Chest. 2007; 132: 1932-8; 3Li et al. Cancer Prev Res (Phila) 2011; 4: 43-50; 4Barr RG et al. AJRCCM. 2007; 176: 1200-7; 5Barr et al. NEJM 2010; 362: 217-27; 6Dransfield et al. COPD 2010; 7: 404-10; 7Ohara et al, Chest 2008; 134: 1244-9; 8Bon et al. AJRCCM 2010 [epub ahead of pring Oct 8]; 9Kurosaki et al, Inter Med 2009; 48: 41-8
Association of Radiographic Emphysema and Airflow Obstruction with Lung Cancer Risk David Wilson,Joel Weissfeld,Arzu Balkan Jeffrey Schragin, Carl Fuhrman, Stephen Fisher,Jonathan Wilson, Jill Siegfried,Steven Shapiro,and Frank Sciurba University of Pittsburgh, ABD GATA, Ankara, Türkiye Am J Respir Crit Care Med Vol 178. pp 738–744, 2008
Objective • To study lung cancer related to radiographic emphysema and spirometric airflow obstruction in tobacco-exposed persons who were screened for lung cancer using chest computed
Method-CT • CT scans are visually scored for emphysema presence and severity. • Scoring procedures used a five level semi-quantitative scale, based on National Emphysema Treatment Trial (NETT) criteria, to represent no, trace, mild, moderate, and severe emphysema.
Results • The study group included 3,638 persons. 57.5 %, no 18.8 %, trace 14.6 %, mild 9.1 % moderate-severe emphysema • The study group included 3,638 persons, %57.3, no %13.6, mild (GOLD I) %22.8, moderate (GOLD II), %6.4 ,severe(GOLD III-IV) airflow obstruction
Results • Ninety-nine lung cancers (2.7 % of 3638) were diagnosed on average 20.9 (0.4-61.8) months after initial screening.
Results • The expected lung cancer risk related to the presence of airflow obstruction GOLD I-IV, OR 2.09, (95% CI 1.33 - 3.27) • Lung cancer risk related to emphysema • OR 3.56 (95% CI 2.21 - 5.73) • After additional adjustments for GOLD class, emphysema remained a strong and statistically significant risk factor (OR 3.14, 95% CI 1.91 - 5.15, p < 0.0001)
Bulgular • Persons with both emphysema and severe airflow obstruction (GOLD III-IV) had the greatest lung cancer risk (adjusted OR 6.29, 95% CI 2.91-13.57)
Conclusion • We have shown that both COPD as measured by GOLD I - IV and emphysema assessed semi-quantitatively on CT scan, are independently related to the risk of developing lung cancer in a high risk population, and that the highest risk is in patients with both COPD and emphysema.
RADIOGRAPHIC PHENOTYPING-THERAPY • Preoperative and postoperative evaluation of emphysema • Bullectomy • Lung Volume Reduction Surgery • Lung Transplantation