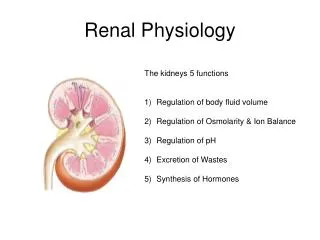
9 December 2009 Renal Physiology
170 likes | 343 Vues
9 December 2009 Renal Physiology. Lab this week: Urinalysis Review website for instructions. Bring handout with Data sheet. Abstracts, Haiku, & Golf Swing. Fig. 14.02a. To be emphasized during Urinalysis Lab. Figure 14.17. Countercurrent Multiplier & Countercurrent Exchange.

9 December 2009 Renal Physiology
E N D
Presentation Transcript
9 December 2009Renal Physiology Lab this week: Urinalysis Review website for instructions. Bring handout with Data sheet. Abstracts, Haiku, & Golf Swing
To be emphasized during Urinalysis Lab. Figure 14.17 Countercurrent Multiplier & Countercurrent Exchange
Misleading diagram! Only 20% is filtered. Inulin (exogenous) and Creatinine (endogenous) used to measure GFR.
Calculating clearance Clearance of s = Urine concentration of s X Urine Volume Plasma concentration of s
Clearance = volume of plasma from which a substance is completely removed (cleared) by the kidneys per unit time. • Clearance of Inulin is 120 ml/min • Cinulin or Ccreatinine = Glomerular Filtration Rate • If C x is greater than GFR ( which is Cinulin) then that substance undergoes NET TUBULAR SECRETION • If C x is less than GFR ( which is Cinulin) then that substance undergoes NET TUBULAR REABSORPTION
Fig. 14.04 Fluid-filled cysts Polycystic Kidney Disease
Fig. 14.10 Apical
Reabsorption and secretion in proximal tubule is NOT under hormonal control. Primary active transport of Na+ establishes a gradient for reabsorption of glucose, amino acids, etc. Reabsorption and secretion in DCT & CCD is under hormonal control. Hormones that act here: ANH, ADH, Aldosterone. Here, reabsorption of Na+ is linked to the secretion of K+.
Glucose & a.a.s Fig. 14.14 Reabsorption of Na+ which begins with Na+/K+ ATPase in basolateral membrane is the first step in reabsorption of most substances. Cl- follows Na+, and these ions create an osmotic gradient in the basolateral clefts which is the driving force for reabsorption of water by diffusion (osmosis) and then bulk flow into peritubular capillaries. Glucose & amino acids
Figure 14.11 If plasma glucose concentration exceeds 200 mg/100 ml, glucose transporters are saturated and any additional filtered glucose will be lost in the urine.
Effect of Aldosterone: insertion of more Na+K+ATPase into basolateral membrane Effect: Increase Na+ reab and Increase K+ Secretion
Figure 14.22 How is secretion of Aldosterone affected by an ↑ plasma volume? Important point: Hormone secretion is not all-or-nothing! Hormone secretion is “graded” and proportional. ↑ plasma volume
Figure 14.30 Apply this information to each of the three Test Beverages used in the Urinalysis Lab! Cell in the adrenal cortex that respond to AII are also receptors for plasma K+ concentration. Sodium reabsorption and potassium secretion are coupled.