Download
1 / 1
10 likes | 114 Vues
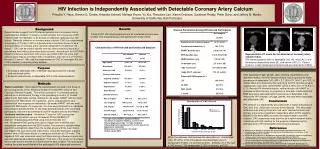
HIV-infected. HIV-uninfected. HIV Infection is Independently Associated with Detectable Coronary Artery Calcium.

E N D
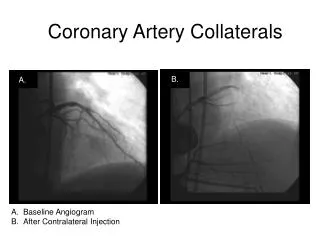
HIV-infected HIV-uninfected HIV Infection is Independently Associated with Detectable Coronary Artery Calcium Priscilla Y. Hsue, Steven G. Deeks, Amanda Schnell, Melissa Krone, Yu Xie, Theodore Lee, Karen Ordovas, Gautham Reddy, Peter Ganz, and Jeffrey N. Martin, University of California, San Francisco Results Background Disease Parameters Among HIV-Infected Participants Recent studies suggest that HIV-infected patients are at increased risk for cardiovascular disease.1 It remains unclear whether this is because of HIV infection itself, its treatment, or an excess of traditional cardiovascular risk factors. Recently, detection of coronary artery calcium (CAC) by computerized tomography (CT scan) in HIV-uninfected persons has been shown to be a strong predictor of coronary artery disease independent of traditional risk factors.2 CAC can be used to identify coronary atherosclerotic plaque at a point where flow limiting obstruction does not exist. According to the ACC/AHA Expert Consensus document, CAC score can predict CAD risk and a high calcium score may be consistent with a moderate to high risk of a CV event in the next 2-5 years.3 We used the measurement of CAC to investigate the role of HIV infection in coronary artery disease. A total of 247 HIV-infected patients and 45 uninfected controls were studied. The characteristics of the patients are shown below. Characteristics of HIV-Infected and Uninfected Subjects A B C Representative CT scans for the detection of coronary artery calcium (CAC) HIV-infected patients with no detectable CAC (A), mild CAC in the left anterior descending artery (B), and severe CAC (C). Patient shown in C later developed symptoms and was referred for CABG. Purpose • To compare detectable CAC in between asymptomatic HIV-infected and uninfected adults • To identify determinants of detectable CAC in HIV-infected patients After adjusting for age, gender, race, smoking, hypertension, and diabetes mellitus, the HIV-infected subjects had a significantly higher prevalence of detectable CAC (OR = 2.7, 95% CI 1.06-6.7, p=0.037). A similar effect was observed when restricting the HIV-infected group to subjects who had never used HAART (OR=3.3; 95% CI 0.77-13.9; p = 0.11). Among HIV-infected subjects, neither duration of HAART or protease inhibitor therapy, or proportion of time with a detectable HIV RNA level were associated with the presence of detectable CAC. Among the HIV-infected, only age, gender, and race were associated with detectable CAC. HIV infection is independently associated with a higher prevalence of CAC and, thus, subclinical coronary artery disease. This effect was observed even among those who had never received antiretroviral therapy, arguing for a treatment-independent effect of HIV infection.Based on this test’s ability to predict coronary events in non-HIV subjects, CAC assessment may prove to be a useful research tool in individuals with HIV infection for the purpose of determining the pathogenesis of HIV-associated coronary artery disease. Methods Patient selection - We studied HIV-infected adults enrolled in the Study of the Consequences of the Protease Inhibitor Era (SCOPE) cohort at San Francisco General Hospital. This cohort consists of 1) untreated patients, defined as no antiretroviral therapy in the preceding 6 months, 2) treated patients with detectable viremia, defined as >24 weeks HAART with the most recent two HIV RNA levels >75 copies/mL, and 3) treated patients who achieved full viral suppression defined as >24 weeks HAART with two most recent HIV RNA levels <75 copies/mL. Controls were obtained from individuals responding to advertisements for the study directed towards HIV-uninfected participants; they were documented to be HIV-negative prior to enrollment. Coronary calcium scans - Multislice CT scan for CAC scoring was performed on all patients using a 16-detector Philips MX8000 CT scanner. Imaging was performed using a slice thickness of 3 mm. Prospective EKG gating was used to trigger axial multislice scan acquisitions using data from the EKG monitor. The scanner’s variable delay algorithm automatically determines the cardiac phase with the least motion and triggers the scan during the least motion. Using this technique, a gantry rotation time of 420 msec results in a temporal resolution of 210 msec. The degree of CAC was measured using the Philips scoring software program and was calculated as described by Agatston.4 The sum of the scores for all arterial lesions was used to provide an overall score for each subject. The radiologists reading the scans were blinded to the participant’s HIV status and treatment. Figure 1 . Serologic Testing for HHV-8 Conclusions Distribution of CAC Scores References • 1. Triant VA, Lee H, Hadigan C, Grinspoon SK. Increased acute myocardial infarction rates and cardiovascular risk factors among patients with human immunodeficiency virus disease. J Clin Endocrinol Metab 2007; 92: 2506-12. • Detrano R, Guerci AD, Carr JJ, Bild DE, Burke G, Folsom AR, et al. Coronary calcium as a predictor of coronary events in four racial or ethnic groups. N Engl J Med 2008,358:1336-1345. • ACC/AHA Writing Group. American College of Cardiology/American Heart Association Expert Consensus Document on Electron-Beam Computed Tomography for the Diagnosis and Prognosis of Coronary Artery Disease. Circulation 2000; 102: 126-40 • 4. Agatston AS, Janowitz WR, Hildner FJ, Zusmer NR, Viamonte M Jr, Detrano R. Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol 1990;15:827-832. When the data was dichotomized into detectable vs. undetectable CAC, 95 (39%) of the HIV patients had detectable calcium compared to 9 (20% ) of controls (p=0.01). Similarly, 41 (17%) had a CAC score > 100 compared to 2 (4%) of controls, p=0.03).