The Complex Shoulder Simplified
540 likes | 736 Vues
The Complex Shoulder Simplified. Manish A. Patel, MD, FAAOS Assistant Professor – Eastern Virginia Medical School Chief of Surgery-Southampton Memorial Hospital (757) 562-7301 www.SouthamptonOrtho.com. Overview. Most mobile joint in body Most dislocated joint Stability Bony articulation

The Complex Shoulder Simplified
E N D
Presentation Transcript
The Complex Shoulder Simplified Manish A. Patel, MD, FAAOS Assistant Professor – Eastern Virginia Medical School Chief of Surgery-Southampton Memorial Hospital (757) 562-7301 www.SouthamptonOrtho.com
Overview • Most mobile joint in body • Most dislocated joint • Stability • Bony articulation • Ligamentous • Muscular
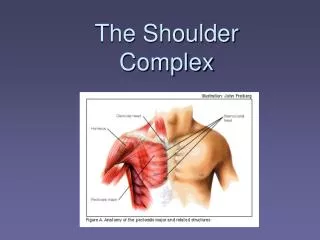
Review of shoulder anatomy • Bones • Scapula • Clavicle • Humeral head • Posterior rib cage • Joints • Sternoclavicular • Acromioclavicular • Glenohumeral • Scapulothoracic
25% humeral head surface in contact with glenoid Joint space thinning seen with OA Humeral head coverage increased to 75% with glenoid labrum Glenohumeral Joint
Labrum • Glenoid Labrum • Dense, fibrous structure • Oval • Deepens glenoid fossa • Stability
Subacromial Space • Bursa • Subacromial space • Source of pain down arm
Rotator cuff muscles • Supraspinatus, infraspinatus, teres minor, subscapularis • Form cuff around humeral head • Keeps humeral head within joint (head depresser) • Abduction, external rotation, internal rotation
Physical Exam • Visualize from front and back • Asymmetry • Pts with rotator cuff tears hold shoulder higher • Atrophy • Sign of chronic glenohumeral joint pathology • Effusions • Shoulder joint can hide a lot of fluid
Active range of motion • Forward flexion • Abduction/adduction • Painful arc of abduction – sensitive, not specific • External rotation • Internal rotation
Passive range of motion • Immobilize the scapula to prevent rotation • Use one arm to push down on shoulder • Use other arm to do the PROM exercises • Abduction • Internal and external rotation • Have arm at patient’s side and abducted to 90 degrees
External Rotation Infraspinatus Teres Minor Physical Exam
Supraspinatus 45 Degrees from front Physical Exam
Impingement Greater Tuberosity under acromion Physical Exam
Cross Arm Test Specific for AC Joint Physical Exam
Biceps Strength Testing • Arms outstretched with palms up at level of shoulder • Forced supination of hand with elbow flexed at 90 degrees • Can be positive for SLAP Test
Trauma Overuse Chronic Previous Surgery Instability Neck Pain Infection Dislocation Frozen Shoulder Etiology of Shoulder Pain
Shoulder Dislocation Fracture Trauma
Fractures – Not all require surgery Surgical options includes (Rods / Plate / Partial vs complete replacement) Treatment
Shoulder Dislocation • Fast Facts • 50 % of ALL dislocations • 95 % anterior • 85 % caused by trauma recur • Posterior think seizures or direct trauma
Shoulder Dislocations • Mechanism? • Anterior vs. posterior • Forced abduction, external rotation, extension • Forced adduction, internal rotation
Shoulder Dislocations • Dislocation vs. Subluxation?
Shoulder Dislocations • Defects following dislocation? • Hill-Sachs • SLAP • Bankart • Rotator Cuff Tear • Fractures
Shoulder Dislocations • Hill-Sachs lesion • Posterior lateral aspect • Compression
Shoulder Dislocation • Superior Labrum Anteroposterior Lesion (SLAP) • Affects biceps
Shoulder Dislocations • Bankart Lesion • Arthroscopic vs. open • Anterior labrum
Unidirectional Multidirectional Instability
Shoulder Dislocations • Chronic Instability – Increasing laxity due to repeat incidents, trauma, genetics, or neuromuscular deficits • Signs and Symptoms • Sport • Clicking • Pain • Weakness
Repetitive Motion Microtrauma Deconditioning Overuse
Impingement Biceps Pathology Arthritis Trauma or Overuse Rotator Cuff Syndrome Frozen Shoulder Chronic Pathology
Impingement syndrome • Compression of rotator cuff tendons and subacromial bursa between greater tuberosity and acromion (type 3) • Repetitive overhead motions • Main cause of rotator cuff tendonitis • Can lead to bursitis, partial or full rotator cuff tears
Rotator Cuff Re-tear Shoulder Stabilization Previous Surgery
Rotator Cuff Tear (Most Common) – Night Pain Pain Radiating up / down Numbness Weakness Decrease Motion 50+ age group RC Tear
Radiology for rotator cuff tears • Interpret carefully • 34% asymptomatic pts (all ages) and 54% pts >60 yo have partial rotator cuff tears • Abnormal rotator cuff signal after trauma may represent strain rather than tear • X-rays • Look for high riding humeral head • Ultrasound • Highly operator dependent • MRI
Tx of rotator cuff tears • Ice, NSAIDs, restrict aggravating motions • Weighted pendulum • No arm slings • Steroid injection • Surgery – refer if young pts, full/large tears, dominant arm • Best if done within 6 weeks • Acromioplasty and debridement
Subacromial Space 22 Gauge needle 1.5” 10 cc total vol. 40 mg kenelog Post placement Aim for Coracoid GH Joint Spinal needle 3” 10 cc total vol. 40 mg Kenelog Straight Aim Posterior placement Beware of Diabetics Injection
Rotator Cuff / Biceps – Good clinical Exam to Start Conservative Options – PT / Injections / Meds Xray and MRI helpful Surgery (Arthroscopic only way to these days in my opinion) Rehab Course Better Treatment
Frozen Shoulder – Diabetics Decrease range of motion in all planes Pain with any motion 40-50 age group Frozen Shoulder
Radiology for adhesive capsulitis • X-rays have limited use • Might see calcifications or degenerative changes that would lead to frozen shoulder • MRI • Enhancement of joint capsule and synovial membrane • 4 mm thickening is 70% sensitive and 95% specific
Tx of adhesive capsulitis • Watchful waiting • Up to 2 years for resolution • Incomplete recovery more likely in pts with DM, or pts with >50% loss of external rotation/abduction • Steroid injection (2 locations) • Manipulation under anesthesia • Aggressive therapy • Pain medication
Biceps tendonitis • Inflammation of long head of biceps • Passes through bicepital groove of anterior humerus • Usually due to repetitive lifting or reaching • Inflammation, microtearing, degenerative changes • Up to 10% pts will have spontaneous rupture • Popeye deformity
Sx of biceps tendonitis • Anterior shoulder pain • Worse with lifting or overhead reaching • Often pts point to bicepital groove • Usually no weakness in elbow flexion
Exam for biceps tendonitis • Bicipital groove tenderness • Look for subacromial impingement • Tendon rupture • Test biceps strength • Yergason test • Elbows flexed with forearms in front • Pt actively resisting external rotation • Tendon may pop out of bicipital groove when downward pressure applied to forearm
Ruptured biceps tendon • Usually rotator cuff tear also present • Get the “popeye” sign • Rarely get significant weakness • Brachioradialis and short head of biceps provide 80-85% elbow flexor strength • Tx is supportive
Tx of biceps tendonitis • Reduce inflammation • Strengthen biceps muscle and tendon • Prevent rupture • Ice, NSAIDs, avoid aggravating motions • 5-10% risk of rupture with noncompliance • Weighted pendulum • Elbow flexion toning exercises • Steroid injection • Surgical referral if sx persist >3 months
Glenohumeral Osteoarthritis • Same risk factors as with OA in other areas • Trauma, obesity, age • Less common than OA in weight bearing joints or spine • Pain, stiffness over months to years • Anterior shoulder is most painful area • Worse with activity • Distinguish from RA, adhesive capsulitis
Exam for Glenohumeral OA • GH joint line tenderness and swelling • Just below coracoid process • Use outward and upward pressure • Effusion may be very hard to see • Decreased ROM • External rotation, abduction • Endpoint stiffness • Crepitus
Joint space narrowing (loss of articular cartilage) Osteophytes Humeral head sclerosis and flattening Club-like deformity Goat’s Beard on X-ray Imaging for glenohumeral OA
Arthritis – From trauma or genetic Conservative – PT (sometimes) / Injections / Meds / Lifestyle modification Surgery – Partial vs Total (Reverse Shoulder) Rehab Treatment
Glenohumeral Joint Infection • Very rare • Increased incidence in diabetics, immuno-compromised patients. • Shoulder looks normal, just bigger. • SEVERE pain. Any motion hurts. • Often a fever. Get labs (CBC, blood cultures, ESR, CRP), XR, then: • Get a consult.