Gout: Its not all crystal clear
560 likes | 1.15k Vues
Gout: Its not all crystal clear. Robert L. Wortmann, M.D. Department of Internal Medicine The University of Oklahoma College of Medicine, Tulsa. But it should be!!!!!!!!. Name another disease that -the cause and pathophysiology are so well undeerstood

Gout: Its not all crystal clear
E N D
Presentation Transcript
Gout:Its not all crystal clear Robert L. Wortmann, M.D. Department of Internal Medicine The University of Oklahoma College of Medicine, Tulsa
But it should be!!!!!!!! Name another disease that -the cause and pathophysiology are so well undeerstood -the diagnosis can be made with such certainty -available therapies can be so effective
Objectives • Review the clinical features of gout • Review the rationale for therapies of gouty arthritis and the underlying hyperuricemia • Answer questions
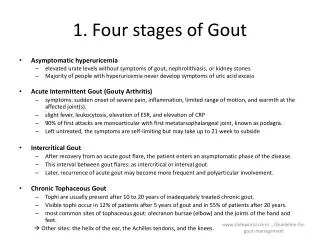
Clinical Features of Gout • Hyperuricemia • Acute Monoarticular Arthritis • Tophi and Chronic Arthritis • Nephrolithiasis
Stage I • Asymptomatic Hyperuricemia • Serum Urate > 7.0 mg/dl
Factors Considered in Therapy of Asymptomatic Hyperuricemia • Renal Disease • Framingham • SMA-12 Autoanalyzer • Antihyperuricemic Medications
Is Hyperuricemia a risk factor for coronary artery disease? • Hyperuricemia is a common feature of the Metabolic Syndrome • Epidemiologic studies are mixed and confusing • Richard Johnson’s rat model of hyperuricemia
Management of Asymptomatic Hyperuricemia • Determine the cause • Address contributing factors • Hypertension • Obesity • Alcoholism • Hyperlipidemia • At this time, specific urate-lowering drugs are not indicated
Stage II • Acute Gouty Arthritis • Intercritical Gout
Overall Gout Prevalence Among All Enrollees 1990-1999 J Rheumatol Aug 2004
Annual Gout Prevalence Among All Enrollees by Age Group 1990-1999 J Rheumatol Aug 2004
Therapy for Acute Gouty Arthritis • Colchicine • Oral • IV • Nonsteroidal Anti-inflammatory Agents • Corticosteroids • Intra-articular • IM (ACTH) • PO
Drug Actions In Acute Gout • Colchicine inhibits • E-selectin mediated PMN adhesion • PMN L-selectin expression • Il-1 expression • Il-8 production • PMN motility • Chemotaxis
Drug Actions In Acute Gout • NSAIDs • Inhibits PGE2 • Corticosteroids • Inhibit PGE2 and LTB4 • Stabilize lysosomal membranes • ACTH • Agonist of the leukocyte melatonin receptor-3
The secret is not what is used, but how quickly therapy is initiated after the attack begins!
Stage III • Chronic Gouty Arthritis • Tophi on physical exam • Chronic degenerative arthritis
Antihyperuricemic Therapy • Treat acute attack until resolved • Colchicine or NSAID for prophylaxis • Xanthine oxidase inhibitor or uricosuric • Address other problems • Hypertension • Obesity • Alcoholism
Goal of Antihyperuricemic Therapy • Serum Urate 5.0 mg/dl! • Lowering serum urate to > 7.0 mg/dl does not reverse the problem. It only slows the rate of progression.
Candidates for Uricosuric Agents • Compliant patients • Under 60 years old • Good renal function* • No ASA • Can use 81 mg but sould be taken 6 hours after the uricosuric • No history of kidney stones • Underexcrete uric acid
Candidates for Allopurinol • Everyone except those • Sensitive to it • Taking azathioprine • Allopurinol has • Once-a-day dosage • Few drug-drug interactions • Effective in renal failure* • Can be used in overproducers and underproducers
Although there have been no new urate-lowering therapies available to treat gout since 1964, there will be soon.
Febuxostat • A nonpurine, selective inhibitor of xanthine oxidase in phase III studies for the treatment of hyperuricemia in patients with gout • Current data support • Potent inhibition with significant urate reduction • Ability to administer in renal insufficiency1 and mild or moderate hepatic insufficiency with no dosage adjustments2 • Safe, effective and well tolerated in limited data of allopurinol intolerant patients3 CH3 OH O H3C N N N CH3 NC NH N S Allopurinol Febuxostat CO2H 1. Swan et al. Arthritis Rheum. 2003;48(9):S529. 2. Khosravan et al. Arthritis Rheum. 2004;50(9):S806. 3. Becker et al. Arthritis Rheum. 2004;50(9):S803.
Febuxostat Phase III Clinical Trial • Study design: randomized, double-blind, 52 week, multicenter trial. • Objective: to assess safety and efficacy (vs. allopurinol) of daily febuxostat administration in lowering sUA levels in subjects with gout and hyperuricemia (sUA 8.0 mg/dL). • Enrollment: N=760 subjects Becker et al. ACR/ARHP Program Book Supplement. 2004;L18.
Febuxostat Phase III Clinical Trial Results Compared to allopurinol, significantly more patients on either dose of febuxostat were able to achieve mean serum urate concentrations less than 6.0 mg/dL Proportion of Subjects with sUA <6.0 mg/dL (ITT Subjects) *p<0.05 for each febuxostat group vs. allopurinol group Becker et al. ACR/ARHP Program Book Supplement. 2004;L18.
Why do people still suffer from gout? • Despite the fact that we understand its cause and underlying pathophysiology • Despite the fact that we can diagnosis it with absolute certainty • Despite the fact that we have such rational and effective therapies
Treatment Failures • Poor prescription • Poor compliance