Download
1 / 39
400 likes | 562 Vues
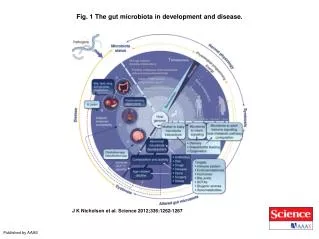
Gut flora in health and disease. Introduction. The intestinal habitat of an individual contains 300–500 different species of bacteria.

E N D
Introduction The intestinal habitat of an individual contains 300–500 different species of bacteria. The stomach and small intestine contain only a few species of bacteria because of the composition of the luminal medium (acid, bile, pancreatic secretion), which kills most ingested microorganisms, and because of the phasic propulsive motor activity towards the ileal end, which impedes stable colonisation of bacteria in the lumen.
By contrast, the large intestine contains a complex high densities of living bacteria. Some of these bacteria are potential pathogens and can be a source of infection and sepsis under some circumstances for instance when the integrity of the bowel barrier is physically or functionally breached. However, the constant interaction between the host and its microbial guests can infer important health benefits to the human host.
Composition of gut flora Colonization of GIT starts immediately after birth and is affected by: • Type of delivery • Type of food • Other environmental factors
Pioneer bacteria can modulate expression of genes in host epithelial cells, thus: • create a favourable habitat for themselves. • prevent growth of other bacteria
Conventional bacteriological analysis of fecal flora Anaerobic Aerobic • Bacteroids - E coli • Bifidobacterium - Enterobacter • Eubacterium - Enterococcus • Clostridia - Klebsiella • Peptocercus - Lactobacillus • Peptostreptocercus - Proteus anaerobic bacteria outnumber aerobic bacteria by a factor of 100–1000.
Functions of gut flora • Metabolic functions: - Fermentation of non digestible dietary residue e.g cellulose and strach by aerobic bacteria short chain FA, source for energy for both host and resident bacteria - Putrefaction of exogenous and endogenous protein (like sloughed epithelium and lysed bacteria) by anerobic bacteria short chain FA as well as toxic substrances like ammonia and amines.
- Production of Vitamin K - Absorption of ions (Fe, Ca, Mg). 2- Trophic functions: - SCFA stimulate epithelial cell proliferation and differentiation, moreover butyrate promote reversion of cells from neoplastic to non neoplastic phentype.
3- Development and homeostatis of immune system: - Specialized epithelial cells (M cells) sample luminal antigens as well as the microflora and transport them to the lymphoid follicles to develop tolerating anti-inflammatory response (Th2 response) through the production of IL10 and TGFB.
- Immunity is constantly reshaped by persistent interactions between the host and its bacteria that take place in the gut. Commensal organisms try to circumvent the immune response by changing its surface antigenicity to allow the organism to escape immunosurveillance and maintain an ecological niche of predominance in the intestinal tract. However, host defences adapt and keep an active control of bacterial growth.
- immune system also can discriminate between potential pathogens from commensal bacteria, with use of a restricted number of preformed receptors i.e. toll-like receptors.
4- Protective function (barrier effect): - compete and adhere to the attachment sites in the brush border of intestinal epithelial. - compete for available nutrients. - produce antimicrobial (bacteriocins). All of this will prevent attachment and subsequent entry of pathogenic bacteria into the epithelial cells
Gut flora and Malabsorption syndrome • In health, motility and acid are the most important factors in keeping the number of bacteria in the upper small bowel low. • Factors predispose to bacterial overgrowth: • Surgical e.g afferent loop syndrome • Anatomical e.g diverticulae, obstruction & fistulae. • Motor e.g scleroderma & DM. • Hypochlohydra e.g atrophic gastritis, post gastrectomy, post vagotomy, PPI.
Consequences of bacterial overgrowth: - Fat malabsorption due to: Bacteria deconjugation of bile acids which allows free bile acids to be reabsorped decrease luminal bile acid concentration limit micelle formation. Patchy mucosal damage by bacteria or toxic effects of FFA -CHO and protein malabsorption due to mucosal damage or bacterial metabolism of these nutrients. - B12 malabsorption: B12 is utilized by the bacteria, in contrast bacteria produces folic acid.
Diagnosis of bacterial overgrowth: - Quantitative culture of luminal contents (gold standard). - Hydrogen breath test. • Treatment: • Treatment of the cause • Antibiotics e.g ciprofloxacin, metronidazole • Stop acid reducing agents • Octerotide improves motility in scleroderma
Gut flora and colorectal cancer Colonic bacteria may initiate cancer through: 1- production of carcinogens from diets rich in meat and fat (nitroso compounds). 2- augmentation of the damage to DNA of colonic cells by dietary carcinogens (heterocyclic aromatic amines found in cooked meat).
High risk of colon cancer was associated with presence of Bacteroides vulgatus and Bacteroides stercoris while, low risk was associated with presence of Lactobacillus acidiphilus, Eubacterium aerofaciens. Although the evidence is not conclusive, colonic flora seem to be a major environmental factor that modulates risk of colonic cancer in human beings.
Gut flora and IBD • In Crohn's disease intestinal T-lymphocytes are hyper-reactive against bacterial antigens, suggest that local tolerance mechanisms are abrogated in such patients. • Increased intestinal mucosal secretion of IgG type antibodies against a broad spectrum of commensal bacteria. unlike normal IgA responses, IgG activate the complement and the cascade of inflammatory mediators
patients with IBD have higher amounts of bacteria attached to their epithelial surfaces than than do healthy people. This causes unrestrained activation of the intestinal immune system • Some patients with Crohn's disease (17–25%) have mutations in the NOD2 gene expressed in macrophages which encodes intracytoplamic receptor for bacterial LPS.
Normally, Interaction of bacterial LPS with NOD2 will lead to activation of NFKB with subsequent production of cytokines and resistance to apoptosis. Mutation in NOD2 gene will lead to diminished macrophage activation in presence of bacterial LPS chronic intracellular infection or failure to develop tolerating immune response in presence of commensal flora.
Faecal stream diversion has been shown to prevent recurrence of Crohn's disease, whereas infusion of intestinal contents to the excluded ileal segments reactivated the mucosal lesions. • In ulcerative colitis, short-term treatment with an enteric-coated preparation of broad-spectrum antibiotics rapidly reduced mucosal release of cytokines and eicosanoids and was more effective in reduction of inflammatory activity than were intravenous steroids.
Gut flora and complications of cirrhosis The gut flora plays a role in the development of infections and also in the hyperdynamic circulatory state of cirrhosis and, although less prominently, it also plays a role in the pathogenesis of hepatic encephalopathy. Bacterial translocation is the key factor in the pathogenesis of SBP and HCS.
Bacterial translocation • Definition: migration of viable micro organisms from the intestinal lumen to mesenteric lymph nodes and other extraintestinal organs. • Conditions associated with BT: • Acute liver failure • Advanced liver cirrhosis • Intestinal ischemia • Intestinal obstruction
Hemorrhagic shock • Burn injury • Acute severe pancreatitis • IBD • Laparotomy & abdominal surgery.
Factors that facilitate BT in cirrhosis: • Impaired immunity: • Cirrhosis is accompanied by decrease in bactericidal activity by phagocytic cells • Decreased hepatic synthesis of complement • Impaired RES activity because of porto-systemic that bypasses the liver and because of impaired phagocytic activity of kupffer cells.
Intestinal bacterial overgrowth: Due to delayed intestinal transit time especially in patients with more severe liver disease. • Intestinal permeability: Cirrhosis is associated with structural and functional alterations in intestinal mucosa that may increase permeability to bacteria.
Gut flora and hyperdynamic circulatory state Vasodilatation, and the subsequent development of the HCS, lead to a worsening of all complications of cirrhosis. Although several vasodilators, such as prostacyclin, adrenomedullin, calcitonin-gene-related peptide, substance P and glucagon have been related to the pathogenesis of HCS, nitric oxide appears to be the key vasodilator responsible for the haemodynamic abnormalities of cirrhosis.
NO is synthesized by different isoforms of NO synthases (NOS); endothelial (e) NOS and neuronal (n) NOS which are expressed constitutively whereas inducible (i) NOS is expressed after induction by LPS, endotoxins and cytokines like the TNF released from GALT in response to translocated gut flora.
Gut flora and hepatic encephalopathy Gut flora contributes to encephalopathy through: - Production of ammonia by urease positive colonic flora. - Production of GABA and benzodiazepine like substances. - H-pylori (urease producing) has controversial role in pathogenesis of HE.
Gut flora and treatment of HE: - Synthetic non-absorbable disaccharides (e.g. lactulose and lactitol) once they reach the colon, bacteria metabolize them, generating organic acids. A lower colonic pH creates an environment hostile to the survival of urease-producing intestinal bacteria and may promote the growth of non-urease-producing lactobacilli. - Non-absorbable antibiotics with activity against urease-producting bacteria (e.g. neomycin, paromomycin) also reduce bacterial ammonia production in the colon and are clinically effective.
Probiotics, Prebiotics & synbiotics • Probiotics: Living microorganisms that up on ingestion exert health benefits beyond those of inherent basic nutrients e.g lactobacilli and bifidobacteria. Recent research expand the definition of probiotics to include genetically engineered microbes and non viable microbes
Prebiotics: Non digestible food indgredients which beneficially affect the host by selectively stimulate the growth and/or the activity of one or limited number of bacteria in the colon having the potential to improve host health. • Synbiotics: A mixture of probiotics and prebiotics which beneficially affects the host.
Probiotics in practice • In diarrheal disease: • Prevention of diarrhea in undernourished children. • Reduce antibiotic associated diarrhea if co-administered with antibiotics. • Shortening of duration of diarrhea in acute gastroenteritis especially those caused by rotavirus. • Through stabilization of indigenous microflora • Through reduction of increased gut permeability • Through enhancement of specific IgA response.
Elemination of lactose intolerance in people who donot efficiently absorb lactose, Lactobacilli provide the enzyme lactase which hydrolyzes lactose. The hydrolyzed lactose is converted to lactic acid. • Prevention of CRC: Putrefactive colonic microflora produce the enzymes convert procarcinogens to carcinogens. Lactobacilli, by competitive inhibition and the production of acidic environment, suppress the metabolic activity of colonic microflora and in this manner may reduce the formation of carcinogens in the large intestine. lactobacilli also suppress carcinogen-induced mutations
Treatment of IBD through: - Production of proteases which degrade the antigenic structure of dietary antigens, an important step in the induction of tolerance to dietary antigens. - Induction of tolerating anti-inflammatory response (Th2 response). - Promoting the normalization of indigenous flora and the exclusion of pathogens.
Treatment of hepatic encephalopathy through: Lactobacilli produce lactic acid creating a gastrointestinal environment which is not suitable for the growth of putrefactive organisms. This results in lower intestinal urease levels and consequently lower blood ammonia levels. In addition, the low pH due to lactic acid production disfavors the absorption of ammonia from the gut into the tissues and facilitates excretion of ammonia from the blood into the gut
Treatment of allergic diseases e.g atopy & food allergy: - Through induction of tolerating anti-inflammatory response (Th2 response). - A significant improvement in the clinical course of atopic eczemahas been observed in infants given a probiotic supplementeddiet, and in parallel, markers of systemic and intestinal allergic inflammation were significantly decreased. Similarresults have been obtained in milk hypersensitive adults.