Download
1 / 55
570 likes | 1.13k Vues
Cardio-Vascular. Anti-lipidemics Statins, Fibrates, Niacin, Omega3, ezetimide… 8/2010 NUR 7755. HYPERLIPIDEMICS. Fats…not water soluble…. Total Chol Trigs. LIPOPROTEINS HDL LDL IDL VLDL Chylo-microns. PEOPLE don’t clog interstate… Chol. and Trigs don’t clog arteries….

E N D
Cardio-Vascular Anti-lipidemics Statins, Fibrates, Niacin, Omega3, ezetimide… 8/2010 NUR 7755
HYPERLIPIDEMICS Fats…not water soluble…. • Total Chol • Trigs • LIPOPROTEINS • HDL • LDL • IDL • VLDL • Chylo-microns PEOPLE don’t clog interstate… Chol. and Trigs don’t clog arteries…
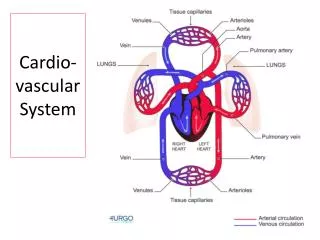
LIPOPROTEINS • HDL • LDL • IDL • VLDL • Chylo-microns lipids vehicles..not people clog highway Each vehicle carries lots of Chol and Trigs (people)
LIPOPROTEINS ligand Chylo-microns VLDL IDL LDL HDL lipophilic Hydrophilic..water soluble
“Cholesterol” Substrates for cell membranes formation hormone synthesis needed for ADEK vit absorption Stored in gb as bile Requires transport protein • Sources: • liver synthesis (20-25%) • intestines • adrenal glands • reproductive organs • animal foods
Cholesterol synthesis • starts w/ 1 molecule of acetyl CoA and 1 molecule of acetoacetyl-CoA => dehydrated to form 3-hydroxy-3-methylglutaryl CoA (HMG-CoA). • => reduced to mevalonate by the enzyme HMG-CoA reductase. • This is the regulated, rate-limiting and irreversible step in cholesterol synthesis and is the site of action for the statin drugs (HMG-CoA reductase competitive inhibitors).
“Triglycerides” • Most dietary fats are “tri” glycerides. • Glycerolmolecule PLUS 3 fatty acid molecules. • triglyceride form not absorbable in duodenum • “pancreatic lipase” enzyme releases the fatty acids • Mono-glycerides & di-glycerides are absorbable • Used as energy source • Require a transport protein
Triglycerides XANTHOMAS SERUM XANTHELASMA
lipoproteins • Total Chol • Trigs • HDL • LDL • IDL • VLDL • Chylo-microns
Chylomicrons Replete w/ dietary trigs ->deliver trigs to skeletal muscle and adipose tissue Large. Contain: apo B 48 (SI) apo B100(liver) apo E 90% trigs Source: dietary fat Life: 12-14hr Catabolized by lipoprotein lipase -> to Chylomicron remnants -> return to liver Free cholesterol liberated Trigs converted to FFA
VLDL/IDL • VLDL Synthesized in liver-> • contain excess Triglyceride (& Cholesterol) not used by the liver for synthesis of bile acids. • contain apolipoprotein B100 and apo E in shell. • =>Secreted by liver-> vessels cleave and absorb trigs -> leave IDL molecules (w/ even more chol) > • Half are taken up by the liver for metabolism into other biomolecules then to LDL • other half continue to lose triacylglycerols in the bloodstream until they form LDL molecules, w/ highest % of cholesterol • Regulated by diet, hormones • Inhibited by chylomicron remnants in liver
Only 1 LDL Lots of Chol Few Trigs ApoB=bad! LDL carries chol to end organs. Receptors recognize Apo B. Remaining LDL-Chol is taken back to liver & degraded Unless: over production, reduced receptors, fat in diet Increased intracellular Chol (from LDL catabolism) inhibits HMG-CoA
HDL Synth. in liver Lots of Chol Few Trigs Apo A=good • Reverse Cholesterol Transport (RCT ) • transport cholesterol back to the liver for excretion • or to other tissues that need cholesterol to synthesize hormones
Lipoprotein separation Apo B Apo B Apo A ..not counted cholesterol..
LDL enters endothelium…oxidized ..macrophage attack..foam cell..plaque.. Lipid cycle
Atherosclerosis Nl……mild……severe……..rupture
I Rare Chylomicrons 250-400 >2500 IIA Common LDL >250 <150 IIB Most common LDL,VLDL >250 150-400 III Rare VLDL remnants 375-500 600-800 IV Common VLDL 225-275 375-500 V Rare Chylomicrons, 350-400 1700-2500 VLDL Fredrickson-Levy-Lees Classification of Hyperlipoproteinemia Lipoprotein Phenotype Occurrence Present in Chol Trig Excess
ADVANCED TESTING GENETIC: Lp(a) ApoE LPA-Aspirin response KIF6-Statin response 9p21-EarlyMI CYP2C19: plavix response ’s coag. ->CVD risk x3. DIET RESPONSE
ADVANCED TESTING INFLAMMATORY MARKERS Lp-PLA2 hsCRP Homocysteine by-product of methionine Vascular inflammation Gen. inflammation OTHER: Insulin Fibrinogen NT-proBNP Q-LDL VIT D Cardiac stress Response to lipid rx
GOALS “National Cholesterol Education Program (NCEP) Adult Treatment Panel III (ATP III)” Risk stratification and treatment guidelines Framingham risk stratification • Lower the LDL (<70-<160) • Lower the non-HDL (30 pt > LDL) • Raise the HDL (>40/50) • Lower the Trigs (<150) LDL: NO risk factors<160 1-2 RF <130 High risk <100
OPTIONS: • Statins • Fenofibrates • Niacin • Omega 3 Fish Oil • Bile Acid Sequestrants • Ezetimide
STATINS: best LDL reduction MOA: inhibits enzyme HMG-CoA reductase Thus: cholesterol synthesis Thus: synthesis of LDL receptors Thus: LDL clearance • USE: LDL • SE: LFTs, myalgias/ rhabdomyositis • CI: antifungals, erythro’s, grapefruit / grapefruit juice inhibit the P4503A4, (lova-, simva-, less w/atorva) • Most Chol produced at night, thus PM dosing
% LDL reduction:6% rule Dosage 10mg 20mg 40mg 80mg • Crestor 46 52 55 • Lipitor 39 43 50 60 • Zocor 30 38 41 47 • Pravachol 22 32 34 37 • Lescol 22 25 36 35 • Mevacor 21 27 31 • Livalo
Statins: examples Potency: $$ Metab./SE T1/2 Prot. Bind. • Crestor H2O sol 2C9/2C19 13-20hr 88% • Lipitor fat sol 3A4 7-14hr 96% • Zocor gen. H2O sol 3A4 2hr 95% • Pravachol $4 fat sol -- 1.8 50% • Lescol fat sol 2C9 1.2 >90% • Mevacor $4 fat sol 3A4 3hr >95% • ??Livalo fat sol 2C9
Red Yeast Rice & Statins • bright reddish-purple fermented rice, which acquires its color from being cultivated w/ the mold Monascus • 1970's researchers in US & Japan were isolating lovastatin from Aspergillus and monacolins from Monascus, (same yeast used to make red yeast rice, but cultured under carefully controlled conditions.) • lovastatin (Mevacor) & monacolin K chemically identical.
Red Yeast rice 1998: FDA banned Cholestin 2001: decision reversed on appeal; FDA sent Warning Letters to companies selling red yeast rice; disappeared x yrs 2003: began to reappear 2007: FDA :consumers should not buy or eat red yeast rice products, may contain an unauthorized harmful drug 2010: 30+ brands available. Many avoid FDA restriction by not having any appreciable moncolin content. Labels / websites say no more than "fermented according to traditional Asian methods" or "similar to that used in culinary applications.” (no mention of cholesterol) If they do not contain/claim to contain lovastatin, and do not make a claim to cholesterol-> not subject to FDA action. monacolin content of red yeast rice dietary supplements can vary widely.
Fenofibrates: MOA Activates “Peroxisome Proliferator Activated Receptor type alpha”(PPARα). • lipolysis & elimination of trig-rich particles • by activating lipoprotein lipase and apo CIII production • PPARα also synthesis of apoproteins AI & AII • VLDL & LDL HDL
Fibrate MOA Activate peroxisome proliferator activated receptor a (PPAR a) • hepatic lipogenesis and VLDL secretion • fatty acid oxidation in liver and muscle • lipoprotein lipase activity • transcription of Apo AI and AII • transfer of phospholipid and chol to HDL • Remodel LDL particles
Fenofibrates… • Generic fenofibric acid 105 • Gen. fenofibrate, micronized 200 w/ meals • Gen. fenofibrate/Triglide/Lofibra 160 • Antara 130 • Fenoglide 120 w/ meals • Fibricor 105 • Lipofen ($25 cash) 150 w/meals • Tricor 145 • Trilipix 135 • Lopid/generic gemfibrozil 600 bid, 30” ac, *caution w/ statin
FENOFIBRATES • USE to :TG (LDL, VLDL, HDL) • SE: GI, rashes, pruritus, urticaria, photosensitivity, myopathy • CI: liver insufficiency, gallstones, RI • gall stones: lithogenicity of bile b/c chol to phosphoipids & bile salts • Feno: creatinine w/o in cr cl • Feno may prevent albuminuria, may induce regression of albuminuria • Hi protein binding ‘s INR w/ coumadin ( coumadin dose 25-35%) • May homocysteine b/c p-par-a • Met: 3A4
PK OF FIBRATES Fenofibrate: Absorbed in intestine hydrolyzed by esterases in intestine to form active metabolite fenofibric acid then hepatic glucuronidation T 1/2 fenofibric acid 20hr (134-200 qd) 60%excreted in urine 25% in feces Gemfibrozil • Absorbed from GI tract • Extensive hepatic conjugation • T !/2 1.5hr • (600 bid ac) • Metabolites excreted in urine
Remember 2 phase metab… Phase 1:oxidation. May involve reduction or hydrolysis of drug • Oxidation is catalysed by CYP450 enzymes and results in the loss of electrons from the drug • resulting drug metabolite is still often chemically active. Fibrates… Phase 2: involves conjugation - • attachment of an ionized group to the drug. • Ionized groups include glutathione, methyl or acetyl • Conjugated w/ hydrophylic substance such as glucuronic acid • …glucuronidation • makes substances more water-soluble,thus, easier elimination through urine or faeces (via bile from the liver). • allows easier transport around the body. • Sometimes less toxic after glucuronidation.
Toxicity Gemfibrozil inhibits glucuronidation and cyp450 metab of statins “Changes in CYP enzyme activity may affect the metabolism and clearance of various drugs. if one drug inhibits the CYP-mediated metabolism of another drug, the second drug may accumulate within the body to toxic levels.” Thus ’sAUC & Cmax of all statins (except fluvastatin) • Thus rhabdomyolysis w/ statin • 33x higher risk w/ cerivaststin/ Baycol • 15x higher risk w/ other statins • Trilipix only one approved for combo use.
Niacin • vitamin B3, nicotinic acid • Other forms of vit B3 : nicotinamide ("niacinamide") • Niacin is converted to nicotinamide • Although identical in vitamin activity, nicotinamide does not have the same pharmacological effects as niacin • Nicotinamide does not reduce cholesterol or cause flushing. • Nicotinamide may be toxic to the liver at doses exceeding 3 g/day for adults.
Niacin Blocks breakdown of fats in adipose tissue • thus ’s FFA’s-> ’s secretion of VLDL and cholesterol by the liver. • By ’ing VLDL levels, niacin also ’s HDL • ’sTC, TG (38%), VLDL, LDL(16%) • HDL (22%) • May lipoprotein(a)
Niacin • Pharmacological doses :1.5 - 6 g/d • SE:flushing, itching,rash, acanthosis nigricans, hyperuricemia (hi dose, exac. gout) • GI: dyspepsia, liver toxicity (>2gm/d, slow release) • Hyperglycemia (hi dose), cardiac arrhythmias • Flush duration 15 -30”, itching sensation • mediated by prostaglandin • blocked by 325mg ASA 30”before or ibuprofen • take w/meals, 8oz liquid • resolves w/2wk, slow titrate • slow- or "sustained"-release forms lessen flush
inositol • dietary supplement, esterified with niacin • sold as "flush-free" or "no-flush" niacin • often marketed and labeled as niacin • misleading consumers into thinking they are getting the active form of the medication. • this form does not cause the flushing • lipid-modifying evidence is contradictory, at best.
Niacin/ Niaspan • AHA & NCEP state: only prescription niacin should be used to treat dyslipidemias • and only under the management of a physician. • Because: niacin at effective intakes of 1500-3000mg/day can also potentially have severe AE. • Monitoring of liver enzymes is necessary.
Niacin options: • Niaspan (Tier 2) 1-2g qhs • start 500 x1mo, by 500 qmo; max 2g/d cyp450 • Slo-Niacin • Nicotinic acid • vit B3 • niacin Make sure it’s nicotinic acid!!
OMEGA 3 • EPA & DHA • stimulate circulation • breakdown of fibrin • blood pressure • trigs • regular intake ‘s Mi risk • MOA:Nutritionally important n−3 fatty acids: • α-linolenic acid (ALA) • eicosapentaenoic acid (EPA) • docosahexaenoic acid (DHA) • All polyunsaturated • Body cannot synthesize n−3 fatty acids • Converts α-linolenic acid to ALA, EPA, DHA • conversions slows if high levels of n−6 fatty acids, • (closely related, derived from linoleic acid)
Omega 3: n−3 & n-6 fatty acids n−6:n−3 fatty acids in oils: canola 2:1 soybean 7:1 Olive 13:1 sunfl(no n−3) flax 1:3 cottonseed (almost no n−3) peanut (no n−3) grapeseed oil (almost no n−3) corn oil 46:1 • 1979: “eicosanoids” discovered: thromboxanes (platelet function), prostacyclins, leukotriene • N6 & N3 compete to be converted to eicosanoids; so ratio of 3:6 affects type eicosanoids produced. • (n−6 converted to pro-inflammatoryprostaglandins) • (N-3: ALA, DHA, EPA) • To control the synthesis of n−6 eicosanoids, consume more n−3
Omega 3: OTC • OTC products claim to contain health promoting 'omega 3', but contain only α-linolenic acid (ALA), not EPA or DHA. • They contain plant oils that must be converted to DHA -> less efficient. • DHA & EPA are made by microalgae in seawater, consumed by fish, accumulate in internal organs.
Foods: cold water oily fish • 7x n3:n6 • Salmon • Herring • Mackerel • Anchovies • sardines • tuna (less n−3) Daily values • Acceptable intake for n−3 is 1.6grams/day for men and 1.1grams/day for women • Higher intakes : protection against CAD • 3g of total EPA/DHA qd safe, no increased risk of bleeding • Perceived risk heavy metal poisoning • Heavy metals selectively bind with protein in the fish flesh rather than accumulate in the oil.
Omega 3: rx Lovaza • Highly purified, more effective • Combination E-EPA / E-DHA • 4gm /d TG 14-30% HDL 10% DI: anticoagulants SE: fish burp (freeze) Monitor: LFTs
OTC:Krill • relatively new source of n−3 fatty acids. • Various claims are made in support of krill oil as a superior source of n−3 fatty acids • B/c less contamination, contain a special antioxidant called astaxanthin. • However, numerous studies have found krill is often contaminated by pollution and astaxanthin hasn't been demonstrated to have a very potent antioxidant capacity
EZETIMIDE MOA: • localizes at brush border of SI • cholesterol absorption • Specifically, binds to a critical mediator of cholesterol absorption, the Niemann-Pick C1-Like 1 (NPC1L1) protein on the GIepithelial cells and hepatocytes • cholesterol absorption leads to an upregulation of LDL-receptors thus LDL-c uptake into cells, thus decreasing plasma levels
Zetia • LDL 18% • 2 major, high-quality clinical trials (2008,2009) showed that it did not improve clinically significant outcomes • panel of experts concluded in 2008 that it should "only be used as a last resort". • Formulations: Zetia10mg, Vytorin (Simva+Zetia) • SE: • HA, diarrhea • Rare: myalgia, LFTs, rash, angioedema, myopathy

![CARDIO-VASCULAR SYSTEM [CVS] FUNCTIONAL ANATOMY OF HEART](https://cdn1.slideserve.com/1739818/cardio-vascular-system-cvs-functional-anatomy-of-heart-dt.jpg)