
JAUNDICE
E N D
Presentation Transcript
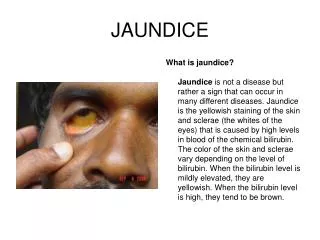
JAUNDICE What is jaundice?Jaundice is not a disease but rather a sign that can occur in many different diseases. Jaundice is the yellowish staining of the skin and sclerae (the whites of the eyes) that is caused by high levels in blood of the chemical bilirubin. The color of the skin and sclerae vary depending on the level of bilirubin. When the bilirubin level is mildly elevated, they are yellowish. When the bilirubin level is high, they tend to be brown.
PHYSIOLOGY OF JAUNDICE Samson Wright Bilirubin comes from red blood cells. When red blood cells get old, they are ingested and destroyed by the RE system( certain phagocyctic cells found in the bone marrow, liver, lymph nodes, spleen and subcutaneous tissue) Normally, about 1% of our red blood cells retire every day, to be replaced by fresh red blood cells. Haemoglobin the chemical in red blood cells that carries oxygen, contains haem attached to globin. In the RE cells the haem part of the molecule is altered by the oxidation of the C of one of its methine (=CH) bridges. The tetrapyrrole ring structure is thus broken and the four pyrrole groups become arranged a s straight chain. As a result of this chemical change the green iron containing compound choleglobin is formed. As its name implies the molecule still contains the original globin. Next both iron and globin are split off and bilirubin is formed. This compound is only soluble in lipid solvents but is extruded into the plasma in a colloid form bound with α-globulin. It is this protein conjugation of bilirubin which is responsible for the solubility of the bilirubin complex in the plasma and which prevents its excretion by the kidneys. On reaching the liver the bilirubin- globulin complex enters the hepatic cells and therein undergo conjugation with glucuronic acid to form water soluble . These compounds pass by the bile ducts into the intestine., where by bacterial degradation, mainly in the colon, stercobilinogn( = urobilinogen) is formed. is formed. Some urobilinogen is reabsorbed and goes via the portal system to the liver, where some escapes into the general circulation and some is re-excreted in the bile. Urobilinogen is water soluble and is filtered off by the kidney and is excreted in the urine.If the urine is allowed to stand urobilinogen is oxidised to urobilin which gives the yellow colour to the urine. The stercobilinogen that is not reabsorbed from the intestine is in excreted in amounts of 20-250mg/day in the faeces. Some of this stercobilinogen is oxidised to stercobilin which is responsible for the yellow colour of the urine.
JAUNDICE- TYPES & CAUSES Jaundice occurs when there is • Excessive breakdown of RBCs resulting in too much bilirubin being produced for the liver to remove from the blood- hemolytic jaundice or prehepatic. (For example, patients with hemolytic anaemia have an abnormally rapid rate of destruction of their red blood cells that releases large amounts of bilirubin into the blood). As bilirubin is not filtered by the kidneys hemolytic jaundice is also called acholuric. • a defect in the liver that prevents bilirubin from being removed from the blood, converted to bilirubin/glucuronic acid (conjugated) or secreted in bile, due to toxic damage, infection of the liver or lack of the enzyme ( glucuronyl transferase) – hepatocellular or hepatic jaundice • blockage of the bile ducts that decreases the flow of bile and bilirubin from the liver into the intestines - Obstructive jaundice or post hepatic. (For example, the bile ducts can be blocked by cancers, gallstones, or inflammation of the bile ducts). The decreased conjugation, secretion, or flow of bile that can result in jaundice is referred to as cholestasis: however, cholestasis does not always result in jaundice.
BILE SALTS These are synthesized by the hepatic cells. Cholic acid is formed from cholesterol and is conjugated with either taurine or glycine to form the bile salts – glcyocholic and taurocholic acids.At the pH of bile 7.3-7.7 taurocholate and glycocholate exist as anions. They are water soluble and are necessary for the digestion of fats. In obstructive jaundice they are regurgitated into blood and are filtered by the kidneys and so are present in urine I
Van den Burgh Test • When a mixture of sulphanilic acid, HCl, and sodium nitrite is added to sierum containing an excess of bilirubin glucuronide a reddish violet colour results max in 30secs. This is called the Direct reaction • When the reagents are mixed with serum containing an excess of bilirubin no colour develops until alcohol is added whereupon the reddish-violet colour appears.
TESTS • Urine – bile salts • Urine – bile pigments-( bilirubin) • Faecal urobilinogen • Faecal fat • LFT • Alkaline phosphatase • Van den Burgh
SICKLE CELL DISEASE • . Sickle cell anemia is an inherited blood disease in which the red blood cells produce abnormal pigment (hemoglobin). The abnormal hemoglobin causes deformity of the red blood cells into crescent or sickle-shapes, as seen in this photomicrograph
JAUNDICE BODY PAIN/JOINT PAIN PAINFUL SWELLINGS TIRED/NOT WORKING POOR GROWTH RECURRENT RESP INFECTION STROKE BLOOD TEST AT GAH WHEN DO YOU SUSPECT SCD AND WHAT SHOULD YOU DO
WHAT TO DO FOR PATIENT WITH SCD • PROTECT AGAINST DIARRHOEA • GIVE PENICILLIN TILL AGE 5 • HYDROXYUREA • GENETIC ADVISE
Dysentery, Amebic dysentery,Cholera, GiardiaEntamoeba histolytica Hepatitis A, Leptospirosis Typhoid fever, Cercarial dermatitis, Cryptosporiosis, Cyclosporiasis, Cysticercosis, Dracunculiasis, Hookworm,, Melioidosis, Neurocysticercosis, Polio, Relapsing fever, Toxocariasis, Trachoma, Traveler's diarrhea, Diseases from contaminated waterHEPATIC JAUNDICE
HEPATATIS A • Hepatitis A is transmitted by contaminated food or water, or contact with a person who is currently ill with the disease. The hepatitis A virus is shed in the stools of an infected person during the incubation period of 15 to 45 days before symptoms occur and during the first week of illness. Blood and other bodily secretions may also be infectious. • The virus does not remain in the body after the infection has resolved, and there is no carrier state (a person or animal that spreads the disease to others but does not become ill). • The symptoms associated with hepatitis A are fever, poor appetite, nausea & vomiting, abd pain ,jaundice & yellow urine. This is because the liver is not able to filter bilirubin from the blood. • Risk factors include having a family member who recently had hepatitis A,
HEPATATIS BCauses, incidence, and risk factors • Hepatitis B is transmitted via blood and other body fluids. Infection can occur through: • Contact with blood in healthcare settings -- this puts physicians, nurses, dentists, and other healthcare personnel at risk • Unsafe sex with an infected person • Blood transfusions • Sharing needles during drug use • Receiving a tattoo or acupuncture with contaminated instruments • Birth -- an infected mother can transmit the virus to the baby during delivery or shortly thereafter
HEPATATIS B • Hepatitis B is also known as serum hepatitis and is spread through blood and sexual contact. It is seen with increased frequency among intravenous drug users who share needles and among the homosexual population. This photograph is an electronmicroscopic image of hepatitis B virus particles. (Image courtesy of the Centers for Disease Control and Prevention.)
HEPATATIS B • In acute hepatitis, it takes about 1-6 months from the time of infection until symptoms appear. Early symptoms may include nausea and vomiting, loss of appetite, fatigue, and muscle and joint aches. Jaundice, together with dark urine and light stools, follows. • About 1% of patients infected with hepatitis B die due to liver damage in this early stage. • The risk of becoming chronically infected, carrier, depends on the person's age at the time of infection. More than 90% of newborns, about 50% of children, and less than 5% of adults infected with hepatitis B develop chronic hepatitis
HEPATITIS B VACCINE • The hepatitis B vaccine is recommended for healthcare workers, people who live with someone with hepatitis B, and others at higher risk. The hepatitis B virus can damage liver cells. Immunization is also recommended for all infants and unvaccinated children & adults
CONCLUSION-CAUSES OF JAUNDICE Sickle cell disease VIRUS/Leptospirosis- in water A in blood B water containing rat urine /faeces ALCOHOL/DRUGS Gallstones