Jaundice
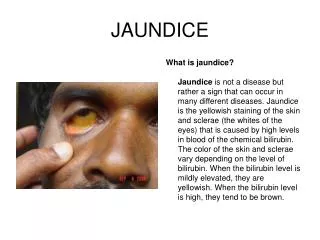
Jaundice . Hannah Leaver. Definition. A yellowish pigmentation of the skin, the conjunctival membranes over the sclerae , and other mucuous membranes caused by hyperbilirubinaemia Detectable clinically when serum bilirubin is > 50μmol/L. Anatomy. Intrahepatic bile ducts ->


Jaundice
E N D
Presentation Transcript
Jaundice Hannah Leaver
Definition • A yellowish pigmentation of the skin, the conjunctival membranes over the sclerae, and other mucuous membranes caused by hyperbilirubinaemia • Detectable clinically when serum bilirubin is > 50μmol/L.
Anatomy • Intrahepatic bile ducts -> • Left and Right hepatic ducts-> • Common hepatic duct-> • Joins cystic duct of GB = Common bile duct -> • Joins pancreatic duct = ampulla of vater/hepatopancreatic ampulla • Enters 2nd part of duodenum when the sphincter of Oddi opens (CCK stimulation etc)
Types of Jaundice • Pre-hepatic • Due to excess bilirubin production e.g. haemolytic anaemia, rhabdomyolysis • ↑unconjugated bilirubin and ↑urobilinogen • Normal urine and stools • Post-hepatic • Impaired excretion of bile from liver to gut • ↑ conjugated bilirubin in blood and urine – dark urine • ↓ conjugated bilirubin in bowel – pale stools
Investigations of Jaundice • History and examination • Dipstick urine (bilirubin) • Blood tests • Macrocytosis, thrombocytopenia or low urea can indicate CLD • Hepatic jaundice = AST/ALT > ALP • Cholestatic jaundice = ALP/GGT > AST • Imaging – biliary tract ultrasound • Evidence of dilated ducts = biliary obstruction -> diagnostic and therapeutic ERCP • MRCP and endoscopic ultrasound • No evidence of obstruction – consider liver biopsy and check auto antibodies
Gall Bladder Disease • Cholelithiasis – Gall Stones • Cholecystitis – Inflammation of Gallbladder • Ascending Cholangitis – Bile duct inflammation • Choledocolithiasis – Gallstone in Common Bile Duct
Cholelithiasis – Gall stones • The presence or formation of gallstones in the gallbladder or cystic duct, resulting from precipitation of cholesterol crystals in supersaturated bile. • Fair, fat, fertile, female of forty • Types of stones • Cholesterol – 20% • Pigmented – 5% • Mixed – 70%
Cholelithiasis • Clinical Features • Asymptomatic • Biliary colic • Cholecystsitis • Cholestatitc jaundice • Pancreatitis • Cholangiocracinoma • Management • Conservative • ERCP • Surgery
Cholecystitis– Inflammation of the gallbladder, secondary to duct obstruction • Symptoms • -RUQ pain – Constant +/- back pain and shoulder tip pain (boas Sign) • -Nausea and vomiting • Signs • tachycardia • Murphy’s sign - elicited by direct palpation of the right upper quadrant.It is characterized by the abrupt arrest of breathing during the inspiration phase due to pain. • Management • NBM • IV fluid • Analgesia • Abx – metronidazole • Definitive treatment Cholecystectomy
Ascending Cholangitis - Cholangitis is an infection of the biliary tract • Causative organisms • E coli, enterococci, klebsiella, proteus, pseudomonas CHARCOT’S TRIAD • Fever • abdo pain (RUQ+/-epigastric) • Jaundice • Management • IV antibiotics (penacillins or cephalosporins) • ERCP if stone apparent
Choledocolithiasis–gall stone in the Common bile duct • Symptoms • RUQ pain – Constant +/- back pain and shoulder tip pain (boas sign) • +/- Epigastric pain • Jaundice • Yellow sclera (sclera icterus) • Nausea and vomiting • Signs • tachycardia • Murphy’s sign
Case Study • 78 yr old female presents as an emergency with upper abdominal pain • Pain on and off over the preceeding months but is getting worse • On admission she is febrile, with a temperature of 39 degress • Pulse is 110bpm • BP 110/70mmHg • Jaundiced, but no other signs of liver disease • Abdo examination reveals diffuse upper abdominal tenderness but no masses
Blood tests • Hb 12.5 g/dL(11.5-16) • WCC 15.7 x 109/L (4-11) • Platelets 172 x 109/L (150-400) • Na 137mmol/L (135-145) • K 3.9 mmol/L (3.5-5) • Urea 8.4 mmol/L (2.5-6.7) • Creatinine 120micromol/L (70-150) • Albumin 30g/L (35-50) • Bilirubin 140micromol/L (3-17) • ALP 450 U/L (30-150) • AST 110 U/L (5-35)
Questions • What diagnosis best describes the patient’s presentation? • What other investigations might be needed urgently? • What would the most suitable treatment be?
Answer 1 • Cholangitis • Charcot’s triad – definitive of infection in the biliary tree. • Not cholecystitis because this refers to inflammation or infection in the gall bladder, not the ducts.
Answer 2 • Ultrasound • Necessary to confirm the presence of stones and demonstrate dilatation of CBD • Necessary to exclude liver abscess
Answer 3 • ERCP • Lithotripsy is not useful in gall bladder or bile duct stones • Open surgery used to be the treatment of choice • ERCP can involve sphincterectomy (cut bile duct open) and stones are extracted with a endoscopic basket or balloon • IV Antibiotics
Case Study • 48 year old female with severe upper abdominal pain • Sudden onset after eating a meal • Epigastric and RUQ pain, coming in waves • Pain causes intense nausea, sweating and retching • Has had a couple of episodes like this previously but nothing quite as intense as this • O/E – patient is in pain with tachycardia, BP 130/85 and temperature of 37.3 • Abdo examination reveals marked RUQ tenderness • No organomegaly or masses
Bloods • Hb13.6 g/dL(11.5-16) • WCC 12.2 x 109/L (4-11) • Platelets 168 x 109/L (150-400) • Na 140mmol/L (135-145) • K 4.2 mmol/L (3.5-5) • Urea 3.8 mmol/L (2.5-6.7) • Creatinine 89micromol/L (70-150) • Albumin 42g/L (35-50) • Bilirubin 12micromol/L (3-17) • ALP 150 U/L (30-150) • AST 24 U/L (5-35)
Questions • What would the next best investigation be? • What should her immediate treatment include?
Answer 1 • Ultrasound • History is typical of biliary colic • USS will show either gallstones or evidence of GB inflammation – thickened GB wall • Look for bile duct dilatation (gall stones in CBD) • Look for focal liver abnormality e.g. abscess
Answer 2 • Management • CONSERVATIVE • Analgesics – biliary pain can be quite resistant to opioids and morphine can exacerbate bile duct spasm • Low fat diet – reduces pain incidence by reducing need for GB contraction • SURGICAL – cholecystectomy • Removes current stones • Reduces risk of bile stasis and further stone formation
Neonatal Jaundice • Day 1 • Concern • Normally haemolysis • Physiological • Day 2-10 • Upper limit of 2 weeks • More common in the breast fed • Immature at conjugating • Low UGT levels • Inhibited by breast milk • Made worse by breast feeding as it de-conjugates bilirubin in the gut • Change from fetal to adult haem • Loss of water after birth • No other pathological features • Unconjugated
Neonatal Jaundice • Prolonged jaundice screen • Occurs/continues after 2 weeks or before day 1 • Unwell with jaundice • Ensure not missing pathology • Conjugated to non conjugated ratio • Manifest • 85 micro-mol/L • Face and eyes first • Gradually spreads to limbs • Worse • Hands and souls
Neonatal Jaundice • Causes • Haemolysis • Blood group incapatability • Rheusus • ABO incompatability • More common the rheusus • Jaundice less severe than in Rheusus • Dehydration • Liver pathology • Hypothyroidism • Infection • Sepsis • Hepatitis • TORCH • Obstructive • Biliary atresia • No connection between biliary tree and gut • Surgery • Neonatal hepatitis • Conjugated • Rare
Neonatal Jaundice • Investigations • Bilirubin levels • Split levels • Liver USS • Thyroid Function • Torch Screen • Urine MSC • Kernicterus • High levels of bilirubin cause it to pass across BBB • Irreversibly stains basal ganglia and causes and encephalopathy • Treated with phototherapy • Changes molecular shape of bilirubin and allows it to be excreted by kidneys • Exchange transfusion • If very high