JAUNDICE
JAUNDICE. By Anfal Gadour. Objectives. Definition of Jaundice Bilirubin Metabolism Investigations Categories Common causes and management. What do you already know?. How would you define jaundice?


JAUNDICE
E N D
Presentation Transcript
JAUNDICE By Anfal Gadour
Objectives • Definition of Jaundice • Bilirubin Metabolism • Investigations • Categories • Common causes and management
What do you already know? • How would you define jaundice? • What is the difference between conjugated and unconjugated bilirubin? • How would you class the different causes of jaundice? • What would you ask about in the history? • What would you look for on examination? • What is corvorsiers law? • What are the most important investigations?
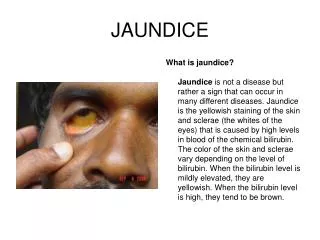
Jaundice (icterus) • Definition: Yellow discoloration of the skin and mucous membranes • Due to increased Bilirubin concentration in the body • Detectable when plasma levels are greater than 50 micromol/l (normal 3-17)
Bilirubin Metabolism • Haemoglobin GLOBIN FE 2+ LIVER BILE SI
Investigations • LFTS: Bilirubin, ALP, AST, ALT, GGT • USS abdo: GB, Cystic Duct, mass • ERCP/MRCP: Stone, Biliary system
Categories • Prehepatic • Hepatic • Posthepatic
Prehepatic • Due to Haemolysiscausing increased bilirubin production • Decreased uptake by liver • Decreased conjugation • unconjugated bilirubin builds up in blood • Water insoluble – therefore doesn’t enter urine • Causes: Physiological (neonates), haemolysis, Gilberts syndrome
Hepatic/Hepatocellular • Hepatocyte Damage • Causes: hepatitis, alcoholic hepatitis, liver cirrhosis, liver metastases, rarer: haemochromatosis, AIH
Posthepatic • Obstructive jaundice • Common bile duct is blocked • Bilirubin overspills into blood – build up of conjugated bilirubin • Water soluble – excreted in urine – dark • Less conjugated bilirubin can reach the bowel – pale stools • If severe – pruritus • Causes: common bile duct stones, pancreatic cancer
Gallstones • Present in 10-20% of population • Cholesterol and mixed • Usually asymptomatic • Risk factors: 4F’s • Complications..
Biliary colic • Pain associated with temporary obstruction of cystic or CBD by a stone • Severe constant pain, subsides over several hours • Pain radiates to right shoulder. Vomiting • Examination normal • Diagnosis: hx, raised ALP and bilirubin. ABSENCE OF INFLAMMATORY FEATURES. • Manage: analgesia, elective cholecystectomy
Acute Cholecystitis • Stone in cystic duct or GB neck • Hx similar to biliary colic. • However, progresses to constant severe pain in RUQ • Fever, tenderness and guarding • Murphys sign • INFLAMMATORY FEATURES – rasied WCC, fever, deranged LFTS, USS • Manage conservatively: NBM, IV fluids, Analgesia, IV abx • Cholecystectomy
Ascending Cholangitis • Infection on biliary tree • Charcots triad – RUQ pain, Fever, Jaundice • Dark urine, pale stools, pruritus • Inv: raised WCC, Blood cultures, Deranged LFTS, USS, CT, ERCP • Manage: Fluid resus, Analgesia, IV abx, ERCP
Pancreatic cancer • Painless Jaundice • Older • Pale stools, dark urine • Weight loss • Palpable GB? • Usually head of the pancreas • Diagnosed on CT • Poor prognosis