Jaundice
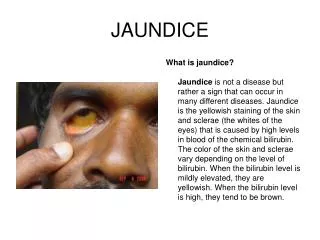
Jaundice. By Saud Al-Sultan Saud Al- Deghaither Abdullah Al- Masoud Supervised by Dr. Faisal Al- Saif. Jundice is an increased concentration of bilirubin in plasma . The normal upper limit is 17 mic mol/L


Jaundice
E N D
Presentation Transcript
Jaundice By Saud Al-Sultan Saud Al-Deghaither Abdullah Al-Masoud Supervised by Dr. Faisal Al-Saif
Jundice is an increased concentration of bilirubin in plasma . • The normal upper limit is 17 mic mol/L • A bilirubin level of 35 mic mol/L or more is usually associated with clinically detectable jaundice , but 17-35 mic mol/L is biochemically jundice . • The excess bilirubin in plasma spills over into the interstitial space causing the tissue become stained yellow .
Classification of jaundice : * Prehepatic ( haemolytic ) : DDx • Congenital : Hereditary spherocytosis , sickle cell disease , thalassaemia . • Acquired : malaria , incompatible blood transfusion .
* Hepatic : DDx • Viral diseases of liver cells e.g. hepatitis (A,B,C,D&E) • Hepatotoxic drugs , such as chlorpromazines . • Cirrhosis . • Gilbert’s disease .
* Posthepatic ( obstructive or surgical jundice ) : • Obstruction in the lumen e.g. gallstones . • Obstruction in the wall of the duct e.g. congenital biliaryatresia,cholangiocarcinoma, postoperative sticture. • Extrisic compression e.g. pancreatitis , pancreatic tumor.
Urine & blood biochemistry in jundice : prehepatic hepaticposthepatic
Symptoms Jaundice (1) onset gradual rapid (2) progression intermittent rapid (3) color changes urine stool (4) pruritus Remember : Jaundice symptoms are secondary to a primary pathology
Pain * painless jaundice * painful jaundice Gall stone pancreatic Fever & Chills infection of bile Wight loss malignancy Personal Hx* alcohol cirrhosis * drugs oral contraceptive chlorpromazine Family Hxcongenital anemia or gall stones Occupation farmers are at high risk of hydated infestation
Signs General signs Abdominal examination Inspection palpation Mass specially spleenomegalyhepatomegaly Percussion ascites shrunken liver Murphy sign
Gall Stones Aetiolgy (1) Cholesterol supra saturation Cholesterol Bile aside lecithin Due to estrogen excess ( obesity , pregnancy , contraceptive) Remember the 5 F
(2) Stasis of bile fasting total parental nutrition (3) Increase Billirubin or deconjugation Bacteria unconjugate the conjugated billirubin or the liver cant conjugate the excess level of billirubin
Asymptomatic 80% Symptomatic Gall bladder (1) cholelithiasis (2) cholecystitis Bile duct (1) choledocholithiasis (2) chlangitis
The Question do all Gall stones cause Jaundice?
CBD Stones Complications' are infection stone formation & pancreatitis
The question know can we have both Jaundice and distended bladder ? YES Courvoisier law state Exceptions' Double stone pathology Mirrizi syndrome
The Investigations • Laboratory Tests • Imaging
Laboratory Tests • CBC: Hb & Hct leukocytosis MCV • Amylas & Lipas • Bilirubin level : Conjugated Vs Non Conjucated • LFTs : ALP , ALT , AST & GGT
Laboratory Tests cont, • ESR • Coagulation Profile : INR • Immunological Tests : Viral antibodies ANA
The Imaging • Plain abdominal X-Ray • Ultrasonography • Radionuclide scan (HIDA scan) • Computed tomography (CT) • Magnetic resonance cholangiography (MRC) • Trance hepatic cholangiogram (PTC) • Endoscopic retrograde cholangiopancreatography (ERCP)
Plain abdominal X-ray • Calcified gallstone • Air in the biliary tree • Air in the gallblader wall or lumen
Arrow points to air within the lumen of GB. • Arrowheads point to air in the GB wall.
U/S • Gallbladder stones 95% sensitivity & specificity • Thickened GB wall • Dilation of intra or extra hepatic ducts • Liver lesions • Pancreatic lesions
These two ultrasound images demonstrate the normal gallbladder in the supine position (above) and decubitus (down).
Gallstones - Acute cholecystitiss • Acute acalculous Cholecystitis
HIDA Scan • uses the radioisotope imino diacetic acid (IDA) to image the biliary system • Technetium-99m-IDA agents IV • When the biliary tract is functioning properly the entire bilirubin pathway from filling of the gallbladder to passage into the common bile duct and duodenum should be visualized. • 90% _ 97% sensitivity & specificity for acute cholecystitis • CCK & Morphin sulfate
This scan indicates normal extraction of bile from the enterohepatic circulation and emptying into the duodenum.
CT • Identifying level and cause of biliary obstruction and imaging neoplasms • identify pathological dilation of the extrahepatic bile ducts • detect pancreatic cancer with 100% accuracy • Liver lesions • Stones in GB & BD
These two CT images demonstrate gallstones within the gallbladder. The CT on the left shows multiple distinct large stones. The axial CT image on the right shows layering of small stones and sludge within the gallbladder
MRC • visualizes the entire gallbladder, biliary tree, and the pancreatic duct. • MRC is a good alternative for those patients who need biliary imaging, but have renal complications or allergy to iodinated contrast media. • MRC images are taken in axial, coronal, and 3-D formats
They demonstrate a portion of the liver and gallbladder. The gallbladder is round and pear-shaped, which is the normal shape of the gallbladder.
This 3-D image of the gallbladder and biliary tree shows good contrast enhancement and flow of bile into the duodenum.
PTC • Dx: Bile duct obstruction Bile leak from duct Obtaining cytology specimen • Rx: Draining obstructed BD Bypassing BDO with stent Extracting BD stone
These two radiographs demonstrate the “skinny needle” used to puncture the bile duct during PTC
ERCP • Dx: BDO Pancreatic duct obstruction Bile leak from ducts • Rx: Draning BDO Bypass BDO Extracting BD stones Performing sphincterotomy
radiograph shows a stricture of the common bile duct • These two fluorospot images taken during an ERCP demonstrates stones in the common bile duct on the left radiograph, and cystic duct on the right radiograph (arrows).
The Management • Depends on the cause • Obstructive or surgical (Gallstones)
Mx of Gallstones • Surgical (cholycystectomy) • Non Surgical: Pharmacological dissolution Mechanical fragmentation : _ ESWL : criteria , < 3 non calcified stones < 3cm in diameter functioning GB
Non Surgical Mx • Asymptomatic pts • Criteria : non-calcified stones < 1cm diameter functioning GB • Agents : ursodeoxycholic acid chenodeoxycholic acid • Tx 6m – 2 years • ½ of pts will have recurrent with in 5 years
Surgical Mx • Cholecystectomy remains the primary procedure for the management of symptomatic gallstone disease.
Mx of Complications • Biliary colic • Acute cholecystitis • choledocholithiasis
Mx Biliary colic • Analgesics & Rehydration • Confirm Dx ( u/s) • Cholecystectomy + Intraobrative cholangiography (IOC)