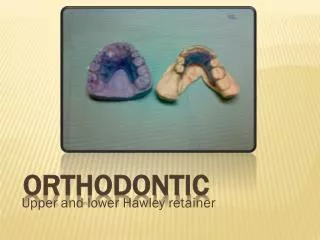
Orthodontic Case Analysis
Orthodontic Case Analysis. Dr. Perucchini Dr. Featheringham Dent 657. THE PROBLEM-ORIENTED APPROACH. Comprehensive way of looking at patient’s problem Involves development of a database Patient interview / questionnaire Clinical exam Diagnostic records.

Orthodontic Case Analysis
E N D
Presentation Transcript
Orthodontic Case Analysis Dr. Perucchini Dr. Featheringham Dent 657
THE PROBLEM-ORIENTED APPROACH • Comprehensive way of looking at patient’s problem • Involves development of a database • Patient interview / questionnaire • Clinical exam • Diagnostic records
I. QUESTIONNAIRE / PATIENT INTERVIEW • Chief complaint • Patient’s subjective assessment of problem • Impaired function vs. impaired esthetics • Establish relative importance of each to the patient
I. QUESTIONNAIRE / PATIENT INTERVIEW • Medical / Dental History • Orthodontic problems are typically a developmental problem, not a pathological problem • Important points on medical history: • Medical problems? • Medications? • Need for prophylaxis? • History of previous trauma? • Important points on dental history: • Hereditary component to malocclusion? • Dental / Orthodontic IQ
I. QUESTIONNAIRE / PATIENT INTERVIEW • Physical Growth Evaluation • Why do we want to evaluate patient’s growth status? • Appropriate referral if problems • Growth modification therapy (headgear) • Rapid growth during adolescence facilitates tooth movement • How can you evaluate a patient’s growth? • Growth charts • Serial cephs • Hand - wrist radiograph • Evaluation of 2° sex characteristics
I. QUESTIONNAIRE / PATIENT INTERVIEW • Physical Growth Evaluation • Why do we want to evaluate patient’s growth status? • Appropriate referral if problems • Growth modification therapy (headgear) • Rapid growth during adolescence facilitates tooth movement • How can you evaluate a patient’s growth? • Growth charts • Serial cephs • Hand - wrist radiograph • Evaluation of 2° sex characteristics
I. QUESTIONNAIRE / PATIENT INTERVIEW • Physical Growth Evaluation • Why do we want to evaluate patient’s growth status? • Appropriate referral if problems • Growth modification therapy (headgear) • Rapid growth during adolescence facilitates tooth movement • How can you evaluate a patient’s growth? • Growth charts • Serial cephs • Hand - wrist radiograph • Evaluation of 2° sex characteristics
I. QUESTIONNAIRE / PATIENT INTERVIEW • Physical Growth Evaluation • Why do we want to evaluate patient’s growth status? • Appropriate referral if problems • Growth modification therapy (headgear) • Rapid growth during adolescence facilitates tooth movement • How can you evaluate a patient’s growth? • Serial cephalograms • Hand - wrist radiograph • Evaluation of 2° sex characteristics
I. QUESTIONNAIRE / PATIENT INTERVIEW • Social / Behavioral Evaluation • Motivation • Internal vs. External • Expectation • Realistic? • Cooperation • Some forms of treatment are cooperation - dependent • May delay treatment altogether, or modify treatment plan to decrease need for patient compliance
II. CLINICAL EVALUATION • Evaluation of Oral Health • Medical and dental problems under control before ortho • Treatment of active caries and perio problems done before ortho • Definitive restorations (crowns) usually not placed until after ortho • Check for mucogingival problems • Often dealt with prior to ortho
II. CLINICAL EVALUATION • Evaluation of Jaw / Occlusal Function • TMJ evaluation • History or TMD? • TMD signs / symptoms? • Evaluation for CR - CO shifts • Presence of shift may alter diagnosis
CO CR
II. CLINICAL EVALUATION • Evaluation of Facial Esthetics • Evaluate facial proportions and symmetry • Disproportion / asymmetry contribute to esthetic problems • FRONTAL VIEW • Symmetry • Dental vs. skeletal midlines • Width of eyes, nose, mouth • Lip competence, gingival display, etc.
II. CLINICAL EVALUATION • Evaluation of Facial Esthetics • Evaluate facial proportions and symmetry • Disproportion / asymmetry contribute to esthetic problems • FRONTAL VIEW • Symmetry • Dental vs. skeletal midlines • Width of eyes, nose, mouth • Lip competence, gingival display, etc.
II. CLINICAL EVALUATION • Evaluation of Facial Esthetics • Evaluate facial proportions and symmetry • Disproportion / asymmetry contribute to esthetic problems • FRONTAL VIEW • Symmetry • Dental vs. skeletal midlines • Width of eyes, nose, mouth • Lip competence
II. CLINICAL EVALUATION • Evaluation of Facial Esthetics • Evaluate facial proportions and symmetry • Disproportion / asymmetry contribute to esthetic problems • FRONTAL VIEW • Symmetry • Dental vs. skeletal midlines • Width of eyes, nose, mouth • Lip competence
II. CLINICAL EVALUATION • Evaluation of Facial Esthetics • Evaluate facial proportions and symmetry • Disproportion / asymmetry contribute to esthetic problems • FRONTAL VIEW • Symmetry • Dental vs. skeletal midlines • Width of eyes, nose, mouth • Lip competence, gingival display, etc.
II. CLINICAL EVALUATION • Evaluation of Facial Esthetics • PROFILE VIEW • Compare vertical thirds • Evaluate position of maxilla and mandible in the anterior - posterior plane • Evaluate lip posture / prominence
II. CLINICAL EVALUATION • Evaluation of Facial Esthetics • PROFILE VIEW • Compare vertical thirds • Evaluate position of maxilla and mandible in the anterior - posterior plane • Evaluate lip posture / prominence
II. CLINICAL EVALUATION • Evaluation of Facial Esthetics • PROFILE VIEW • Compare vertical thirds • Evaluate position of maxilla and mandible in the anterior - posterior plane • Evaluate lip posture / prominence
RETROGNATHIC PROGNATHIC
II. CLINICAL EVALUATION • Evaluation of Facial Esthetics • PROFILE VIEW • Compare vertical thirds • Evaluate position of maxilla and mandible in the anterior - posterior plane • Evaluate lip posture / prominence
III. ANALYSIS OF DIAGNOSTIC RECORDS-CAST ANALYSIS-CEPH ANALYSIS
CAST ANALYSIS • Asymmetry • Often due to early loss of primary tooth on 1 side of arch
CAST ANALYSIS • Molar Classification
CAST ANALYSIS • Space available vs. space required • Permanent Dentition • Measure the M-D width of teeth and compare to arch length • Mixed Dentition • Need width of unerupted canines and premolars • Tanaka - Johnston or Moyers Analysis • Use width of erupted lower incisors to predict
CEPH ANALYSIS • To identify pathology • To define anatomic basis for malocclusion • To evaluate changes due to treatment and growth
CEPH ANALYSIS • To identify pathology • To define anatomic basis for malocclusion • To evaluate changes due to treatment and growth
CEPH ANALYSIS • To identify pathology • To define anatomic basis for malocclusion • To evaluate changes due to treatment and growth
ORTHODONTIC CLASSIFICATION SYSTEMS • Angle • First system to define normal occlusion • Defined three classes of malocclusion • Weakness: No information about transverse or vertical relationships • Ackerman / Proffit • Describes five major characteristics of malocclusion