Download
1 / 39
920 likes | 4.54k Vues
Coarctation of Aorta. Seoul National University Hospital Department of Thoracic & Cardiovascular Surgery. Coarctation of Aorta. 1. Definition A congenital narrowing of upper descending thoracic aorta adjacent to the site of attachment of ductus arteriosus 2. History

E N D
Coarctation of Aorta Seoul National University Hospital Department of Thoracic & Cardiovascular Surgery
Coarctation of Aorta • 1. Definition • A congenital narrowing of upper descending thoracic aorta • adjacent to the site of attachment of ductus arteriosus • 2. History • Morgagni : 1st description in 1760 • Bonnett : postductal & preductal type in 1903 • Crafoord : 1st coarctation repair in 1944 • Vorsschulte : prosthetic onlay graft or vertical incision • and transverse closure in 1957 • Waldhausen : subclavian patch aortoplasty in 1966
Coarctation of Aorta • Developmental factor • 1. Underdevelopment or hypoplasia of aortic • arch or isthmus Definition of hypoplasia • * Proximal arch : 60% of ascending aorta • * Distal arch : 50% of ascending aorta • * Isthmus : 40% of ascending aorta • 2. Presence of ectopic ductal tissue in the aorta
Aortic Arch Hypoplasia • Definition • Hypoplastic arch has higher ratio of elastin lamellae to vessel diameter & increase in collagen and decrease in alpha-actin-positive cell that may hinder the ability of arch to distend. 1. 50% reduction of terminal end of ascending aorta, sometimes, because of small ascending aorta in coarctation, descending thoracic aorta is compared. 2. Transverse arch diameter less than body weight in Kg plus 1 3. Z-value less than –2 or more
Coarctation of Aorta • Morphology 1. Localized stenosis • * More than 50% reduction in cross sectional area • * Shelf, projection, infolding of aortic media into the • lumen opposite the ductus arteriosus • * Usually intimal hypertrophy ( intimal veil ) extends • the shelf circumferentially and further narrows the • lumen (Rodbard) 2. Tubular hypoplasia • * Severe with lesser narrowing • * Proximal aortic & arterial wall • * Distal aortic arch narrowing • * Fetal flow pattern (Rudolph)
Coarctation of Aorta • Evolution
Coarctation of Aorta • Pathophysiology • Narrowed aorta produces increased left ventricular afterload and wall stress, left ventricular hypertrophy, and congestive heart failure. • Systemic perfusion is dependent on the ductal flow and collateralization in severe coarctation
Coarctation of Aorta • Associated pathology • 1. Collateral circulation • * Inflow : primary from branches of both subclavian arteries • . internal mammary artery . vertebral artery • . costocervical trunk . thyrocervical trunk • * Outflow : into descending aorta, two pairs of intercostal arteries • 2. Aneurysm formation of intercostal arteries • * 3rd, & 4th rib notching * rare before 10 years of age • 3. Coronary artery dilatation and tortuosity • * due to LVH • 4. Aortic valve • * bicuspid (27-45%) * stenosis ( 6 - 7%) • 5. Intracranial aneurysm • * berry type intracranial aneurysm in some patients • 6. Associated cardiac anomaly • * 85% of neonates presenting COA
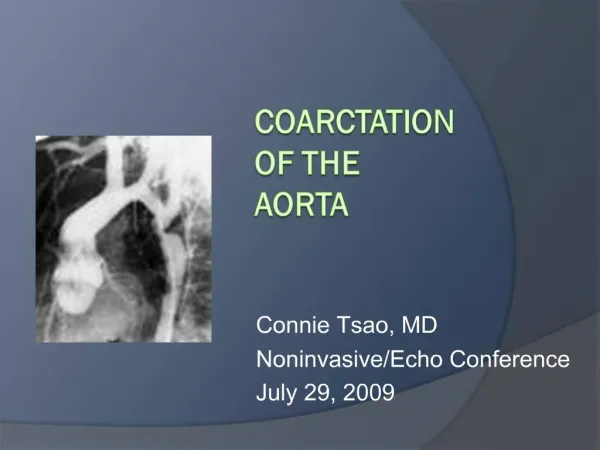
CoA Tubular Hypoplasia Distal arch PDA
Coarctation of Aorta • Natural history • 1. Incidence • * 5-8% of CHD (5 per 10000 live births) • * Isolated CoA (82% of total CoA) ; male:female = 2:1 • CoA + VSD 11%, COA + other cardiac anomalies 7% • * Complex CoA ; no sex difference • 2. Survival of pure CoA • * 15% : CHF in neonate or infancy • * 85% : survive late childhood without operation • * 65% : survive 3rd decade of life (2% at 60 years) • 3. Bacterial endocarditis : common in 1st 5 decades • 4. Aortic rupture : 2~3rd decade • 5. Intracranial lesion : subarachnoid hemorrhage(cong. Berry • aneurysm)
Coarctation of Aorta • Clinical features & diagnosis • 1. Infancy • 1) Closure of ductus (7-10 days) produces severe obstruction • 2) Ductus arteriosus remains patent - differential cyanosis • 3) Associated intracardiac defect - more severe, early onset • 4) Degree of collateral circulation • 2. Childhood • * Asymptomatic without significant associated lesion • * Hypertension (90%) * Cardiomegaly (33%) • * Rib notching (15%) • 3. Adolescence and adult • * Hypertension ; very common * Valvar heart disease • * Heart failure at 30 years of age • 4. Associated syndrome • * Turner syndrome (XO) : 2% * Von Recklinghausen’s D • * Noonan’s syndrome or congenital rubella
Coarctation of Aorta • Indications for operation • 1. Reduction of luminal diameter greater • than 50% at any age • 2. Upper body hypertension over 150mmHg • in young infant ( not in heart failure ) • 3. CoA with congestive heart failure • at any age
Coarctation of Aorta • Techniques of operation • 1. Subclavian flap aortoplasty • Neonate, infant and child up to 10 years • 2. End-to-end anastomosis • Preferred in any age group • * Extended end-to-end anastomosis • * Radically extended end-to-end anastomosis • 3. Patch angioplasty or graft replacement
Prevention of Recoarctation • Ideal operative procedure • Successfully address transverse arch hypoplasia (if present), • Resection of all ductal tissue, and • Prevention of residual circumferential scarring at the aortic anastomotic sit. • Factors • Younger age at operation • Presence of aortic arch hypoplasia remain risk factors for recoarctation
Regional Cerebral Perfusion • Technique • We begin full-flow CPB at a calculated baseline of 150 mL · kg–1 · min–1 and, after snare placement on the proximal brachiocephalic vessels, initiate RLFP by reducing pump flow to 50% of baseline. • We make further adjustments such that baseline cerebral blood flow velocity as measured by transcranial Doppler and cerebral oximetrics as measured by NIRS are optimally maintained. • RLFP provides consistent cerebral circulatory support and that this support is bilateral, despite being applied to the inominate artery.
Pediatric Cardiac Surgery • Neurologic complications • Incidence of 2.3% for overt clinicalpresentation & up to 60% when sensitive magneticresonance imaging is applied in heart surgery of infants & children. • In control of the arch proximal to theleft carotid artery, during COA surgery, this assumes that collateral blood flow and completenessof the circle of Willis allows for a favorable and even distributionof cerebral blood flow. • But patients undergoingcoarctation repair, proximal occlusion of the aortic arch resultsin transient but significant impairment in contralateral cerebraloxygen balance
Blood Supply to Spinal Cord The most important blood supply to spinal cord comes from spinal artery, a minor supply is from Adamkiewicz artery
Coactation of Aorta Resection & Extended end-to-end Anastomosis
Coarctation of Aorta Enlargement of VSD, Resection of Conal Septum
Coarctation of AortaEnd-to-Side Anastomosis Opening of Resected Segment
Coactation of Aorta • Operative results • Hospital mortality Causes of early death are acute and chronic cardiac failure or severe pulmonary insufficiency • Incremental risk factor for death 1) Older age 2) Hypoplastic left heart class 3) Techniques of operation
Coactation of Aorta • Operative results • Mobidity • 1) Paraplegia (0.2 ~ 1.5%) • 2) Hypertension and abdominal pain • 3) Persistent or recurrent coarctation • - more than 20mmHg • - high incidence in young • 4) Upper body hypertension without resting gradient • - increased vascular activity in the forearm • - age at operation is risk factor • 5) Late aneurysm formation • - higher in onlay patch technique • 6) Valvular disease • 7) Congestive heart failure with hypertension • 8) Bacterial endocarditis
Coactation of Aorta • Special features of postoperative care • 1. Systemic arterial hypertension • Usually, but infant or young child doesn’t • need to be treated. • 2. Abdominal pain • Usually mild abdominal discomfort for a few days, • and prominent in 5 - 10%. • Control hypertension, nasogastric decompression, • IV maintain • 3. Chylothorax • 5%
Coactation of Aorta Repair • Postoperative hypertension • Sealy Altered baroreceptor response with increased excretion of epinephrine or norepinephrine • Rocchin Sympathetic nervous system in early phase, and renin-angiotensin system in late phase
Coactation of Aorta Repair • Paraplegia • 1. Duration of spinal cord ischemia • 2. Duration of intercostal artery ischemia • 3. Intraoperative proximal hypotension • 4. Postoperative hypotension • 5. Hyperthermia during operation • 6. Anastomosis with tension • 7. Acidosis in the perioperative periods
Coactation of Aorta • Special situation & controversies • 1. CoA proximal to left subclavian artery • * 1% of all COA • * reverse subclavian flap • * abdominal CoA : 0.5 ~ 2% • 2. Mild or moderate coarctation • * degenerative change prone to occur • 3. Prevention of paraplegia • * Collateral circulation, hypothermia(< 45min at 33 deg C) • * Descending aortic pressure under 50mmHg after clamp • 4. Recurrent coarctation • Increased mortality and morbidity • 5. CoA with VSD or other anomalies • Increased mortality and morbidity
Coactation of Aorta • Balloon dilatation • The roleof balloon dilatation is controversial because of early restenosis,the need for multiple interventions, potential limb ischemia,and the increased risk of aneurysm formation • The mechanism for early restenosis in neonates may be related to multiple factors including ductal tissue constriction orrecoil, isthmus hypoplasia, intimal hyperplasia as a resultof smooth muscle cell proliferation, and matrix protein productionwith arterial remodeling are involved in restenosis