Download
1 / 48
1.11k likes | 2.54k Vues
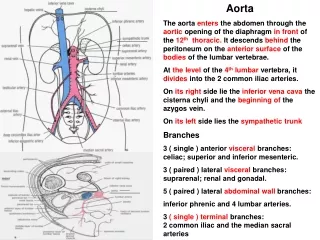
PERIPHERAL ARTERY DISEASE VENOUS THROMBOSIS . Diseases of the Aorta. Yaser Jenab, MD Assistant Professor of Cardiology . Tehran Heart Center. Aortic Wall. Thin intima composed of: Endothelium, Subendothelial connective tissue, And an internal elastic lamina;

E N D
PERIPHERAL ARTERY DISEASE • VENOUS THROMBOSIS Diseases of the Aorta Yaser Jenab, MD Assistant Professor of Cardiology Tehran Heart Center
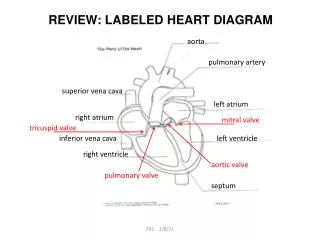
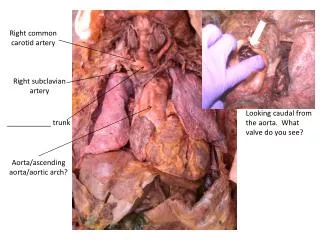
Aortic Wall • Thin intima composed of: • Endothelium, • Subendothelial connective tissue, • And an internal elastic lamina; • Thick tunica media composed of: • Smooth muscle cells • And extracellular matrix; • Adventitia composed of: • Connective tissue • Vasavasorum • And nervivascularis
Aortic Aneurysm • An aneurysm is defined as a pathologic dilation of a segment of a blood vessel. • TRUE ANEURYSMinvolves all three layers of the vessel wall • PSEUDOANEURYSM, in which the intimal and medial layers are disrupted and the dilated segment of the aorta is lined by adventitia only
Aortic Aneurysms • Abdominal • Thoracic • Thoracoabdominal
Etiology Aortic aneurysms result from conditions that cause: Abnormal production of the structural components of the aortic wall: elastin and collagen Degradation
Degenerative Aortic Aneurysms • The most common pathologic condition associated with degenerative aortic aneurysms is atherosclerosis. • Many patients with aortic aneurysms have coexisting risk factors for atherosclerosis, as well as atherosclerosis in other blood vessels
Cystic Medial Necrosis • Degeneration of collagen and elastic fibers in the tunica media of the aorta • Affects the proximal aorta, • Leads to the development of fusiform aneurysms involving the ascending aorta and and the sinuses of valsalva
Thoracic Aortic Aneurysms • Cystic medial necrosis is the most common pathology associated with ascending aortic aneurysms, • Atherosclerosisis the condition most frequently associated with aneurysms of the aortic arch and descending thoracic aorta.
Thoracic Aortic Aneurysms • The risk of rupture is related to the: • Size of the aneurysm • Presence of symptoms, • Most thoracic aortic aneurysms are asymptomatic; however, compression or erosion of adjacent tissue by aneurysms may cause symptoms such as • chest pain, • shortness of breath, • cough, • hoarseness, and dysphagia. • Compression of the superior vena cava may produce congestion of the head, neck, and upper extremities. • Aortic regurgitation,
DiagnosisThoracic Aortic Aneurysms • Chest x-ray • Echocardiography, particularly transesophageal echocardiography, • Contrast-enhanced CT, • Magnetic resonance imaging (MRI), • And conventional invasive aortography • In asymptomatic patients whose aneurysms are too small to justify surgery, noninvasive testing with either contrast-enhanced CT or MRI should be performed at least every 6–12 months to monitor expansion.
TreatmentThoracic Aortic Aneurysms • Adrenergic blockers • Control hypertension • Angiotensinrenzymeeceptor antagonists and angiotensin-converting inhibitors • Operative repair with placement of a prosthetic graft is indicated in patients with symptomatic thoracic aortic aneurysms, those in whom the ascending aortic diameter is >5.5–6 cm or the descending thoracic aortic diameter is >6.5-7 cm, and those with an aneurysm that has increased by >1 cm per year. In patients with marfan syndrome or bicuspid aortic valve, ascending thoracic aortic aneurysms >5 cm should be considered for surgery. • Endovascular repair is an alternative treatment for some patients with descending thoracic aortic aneurysms.
Abdominal Aortic Aneurysms • More frequently in males than in females • The incidence increases with age. • At least 90% of all abdominal aortic aneurysms >4.0 cm are related to atherosclerotic disease, • The risk of rupture increases with the size of the aneurysm • The formation of mural thrombi within aneurysms may predispose to peripheral embolization.
Abdominal Aortic Aneurysm • Commonly produces no symptoms. • It usually is detected on • Routine examination as a palpable, pulsatile, expansile, and nontender mass, • Or it is an incidental finding observed on an abdominal x-ray or ultrasound study performed for other reasons. • As abdominal aortic aneurysms expand they may become painful. • Aneurysmal pain is usually a harbinger of rupture and represents a medical emergencywhich requires an emergency operation.
Abdominal Aortic Aneurysm • Abdominal ultrasound • Screening by ultrasonography is recommended for men age 65–75 years who have ever smoked. • Should be considered for screening for abdominal aortic aneurysms • Siblings or offspring of persons with abdominal aortic aneurysms, • Individuals with thoracic aortic or peripheral arterial aneurysms, • CT with contrast and MRI are accurate noninvasive tests to determine the location and size of abdominal aortic aneurysms and to plan endovascular or open surgical repair
TreatmentAbdominal Aortic Aneurysms • Expanding rapidly or • Associated with symptoms. • >5.5 cm • Operative repair of the aneurysm with insertion of a prosthetic graft • Or endovascular placement of an aortic stent graft :
Acute Aortic Syndromes • Aortic rupture • Aortic dissection, • Intramural hematoma, • And penetrating atherosclerotic ulcer
Aortic Dissection • The initiating event is either • A primary intimal tear with secondary dissection into the media • Or a medial hemorrhage that dissects into and disrupts the intima. • The pulsatile aortic flow then dissects along the elastic lamellar plates of the aorta and creates a false lumen.
Predisposing Factors Aortic Dissection • Systemic hypertension, a coexisting condition in 70% of patients, • cystic medial necrosis • Marfan syndrome • Ehlers-danlos syndrome. • Takayasu'sarteritis, giant cell arteritis, • Bicuspid aortic valve, • Coarctation of the aorta, • History of aortic trauma • During the third trimester of pregnancy.
Clinical Manifestations • The presentations of aortic dissection are the consequences of • Intimal tear, • Dissecting hematoma, • Occlusion of involved arteries, • compression of adjacent tissues. • Acute aortic dissection presents with • The sudden onset of pain: very severe and tearing and is associated with diaphoresis. • The pain may be localized to the front or back of the chest, often the interscapular region, and typically migrates with propagation of the dissection. • Other symptoms include syncope, dyspnea, and weakness.
Clinical Manifestations • Dissection occluding the major arteries causing: • Bowel ischemia, • Hematuria, • And myocardial ischemia • Compression of adjacent structures by the expanding dissection causing aneurysmal dilation • Superior cervical ganglia, • Superior vena cava, • Bronchus, • Esophagus • Hemopericardium and cardiac tamponademay complicate a type A lesion with retrograde dissection. • Acute aortic regurgitation is an important and common (>50%) complication of proximal dissection
Aortic dissection • Chest x-ray : • Widened superior mediastinum • Pleural effusion (usually left-sided) • An ECG that shows no evidence of myocardial ischemia • Echocardiography, TEE • CT • MRI
TreatmentAortic Dissection • Medical • Adrenergic blockers to achieve a heart rate of approximately 60 beats/min • Sodium nitroprusside infusion to lower systolic blood pressure to ≤120 mmhg. • Labetalol • Emergent or urgent surgical correction • Acute ascending aortic dissections • Intramural hematomas (type A) • Complicated type B dissections, including those characterized by • Propagation, • Compromise of major aortic branches, • Impending rupture, • Or continued pain.
Peripheral Artery Disease(PAD) • A clinical disorder in which there is a stenosis or occlusion in the aorta or the arteries of the limbs. • Atherosclerosis is the leading cause of PAD in patients >40 years old. Other causes include: • Thrombosis, • Embolism, • Vasculitis, • Fibromuscular dysplasia, • Entrapment, • Cystic adventitial disease, • Trauma • Atherosclerotic lesions occur preferentially at arterial branch points,
Clinical Evaluation(PAD) • Fewer than 50% of patients with PAD are symptomatic • The most common symptom is intermittent claudication, which is defined as a pain, ache, cramp, numbness, or a sense of fatigue in the muscles; • it occurs during exercise and is relieved by rest. • The site of claudication is distal to the location of the occlusive lesion
Physical Findings(PAD) • Decreased or absent pulses distal to the obstruction, • Muscle atrophy. • With more severe disease: • Hair loss, • Thickened nails, • Smooth and shiny skin, • Reduced skin temperature, • And pallor or cyanosis • In patients with critical limb ischemia, ulcers or gangrene may occur
Diagnosis (PAD) • Ankle:brachial index(ABI) is • 1.0 in normal individuals • <1.0 in patients with PAD • <0.5 is consistent with severe ischemia. • Duplex ultrasonography , • Performed before potential revascularization : • Magnetic resonance angiography (MRA), • Computed tomographic angiography (CTA), • Conventional contrast angiography
Treatment (PAD) • Reduce the risk of associated cardiovascular events, discontinuing cigarette smoking • Therapies for intermittent claudication and critical limb ischemia include: • Supportive measures: • care of the feet , • exercise regularly • Medications: • cilostazol, • pentoxifylline • Catheter-based and surgical interventions
ThromboangiitisObliterans(Buerger's disease) • An inflammatory occlusive vascular disorder • Involving small and medium-size arteries and veins in the distal upper and lower extremities. • This disorder develops most frequently in men <40 years of age. • There is a definite relationship to cigarette smoking
Acute Arterial Occlusion • Results in the sudden cessation of blood flow to an extremity. • The severity of ischemia and the viability of the extremity depend on • The location • Extent of the occlusion • The presence and subsequent development of collateral blood vessels. • There are two principal causes of acute arterial occlusion: • Embolism • And thrombus in situ.
Sources Of Arterial Emboli Acute Arterial Occlusion • Cardiac disorders that cause thromboembolism include • Atrial fibrillation • Acute myocardial infarction; • Ventricular aneurysm; • Cardiomyopathy; • Endocarditis; • Thrombi associated with prosthetic heart valves; • Atrialmyxoma. • Aneurysms of the aorta and large vessels • Arterial emboli tend to lodge at vessel bifurcations
Clinical FeaturesAcute Arterial Occlusion • Severe pain, paresthesia, numbness, and coldness develop in the involved extremity within 1 hour. • Paralysis may occur with severe and persistent ischemia. • Physical findings • Loss of pulses distal to the occlusion • Cyanosis or pallor, • Mottling, • Decreased skin temperature, • Muscle stiffening, • Loss of sensation, • Weakness, and/or absent deep tendon reflexes.
TreatmentAcute Arterial Occlusion • Heparin • In cases of severe ischemia of recent onset immediate intervention: • Endovascular or surgical thromboembolectomy • Or arterial bypass procedures • Intraarterial thrombolytic therapy • When acute arterial occlusion is caused by a thrombus in an atherosclerotic vessel or arterial bypass graft. • Thrombolytic therapy may also be indicated when the patient's overall condition contraindicates surgical intervention • Or when smaller distal vessels are occluded, thus preventing surgical access • Amputation is performed when the limb is not viable, as characterized by loss of sensation, paralysis, and the absence of doppler-detected blood flow in both arteries and veins.
Atheroembolism • A subset of acute arterial occlusion. • Multiple small deposits of fibrin, platelets, and cholesterol debris embolizefrom proximal atherosclerotic lesions or aneurysmal sites. • Large protruding aortic atheromasare a source of emboli that may lead to • Stroke • Renal insufficiency • Limb ischemia. • Atheroembolism may occur after intraarterial procedures. • Distal pulses usually remain palpable. • Digital vascular occlusion may result in ischemia and the "blue toe" syndrome
Venous Thrombosis(thrombophlebitis ) • The presence of thrombus within a superficial or deep vein, along with the accompanying inflammatory response in the vessel wall • The factors that predispose to venous thrombosis were initially described by Virchow • Stasis, • Vascular damage, • Hypercoagulability.
Superficial Vein Thrombosis • Does not result in pulmonary embolism. • It is associated with • Intravenous catheters and infusions, • Occurs in varicose veins, • Migrating superficial vein thrombosis is often a marker for a carcinoma
Clinical Features And Treatment Superficial Vein Thrombosis • Pain localized to the site of the thrombus. • Examination reveals a reddened, warm, and tender cord extending along a superficial vein. • The surrounding area may be red and edematous. • Treatment • Bed rest with leg elevation and application of warm compresses. • NSAIDs may provide analgesia • If a thrombosis of the greater saphenous vein develops in the thigh and extends toward the saphenofemoral vein junction, it is reasonable to consider anticoagulant therapy to prevent extension of the thrombus into the deep system and a possible pulmonary embolism.