Download
1 / 66
741 likes | 1.24k Vues
Diseases of the Aorta. Oh’s The Echo Manual. Aortic aneurysm Aneurysm of the sinus of Valsalva Atherosclerosis & aortic debris Aortic dissection & intramural hematoma Aortitis Coarctation of the aorta. Feigenbaum’s Echocardiography. Aortic dilatation & aneurysm Valsalva sinus aneurysm

E N D
Oh’s The Echo Manual • Aortic aneurysm • Aneurysm of the sinus of Valsalva • Atherosclerosis & aortic debris • Aortic dissection & intramural hematoma • Aortitis • Coarctation of the aorta
Feigenbaum’s Echocardiography • Aortic dilatation & aneurysm • Valsalva sinus aneurysm • Aortic dissection • Aortic atheroma • Miscellaneous conditions
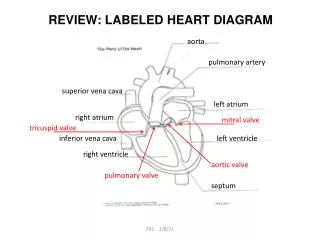
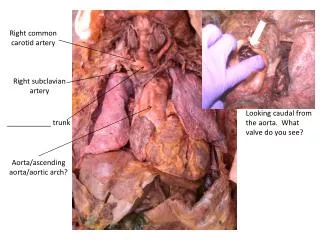
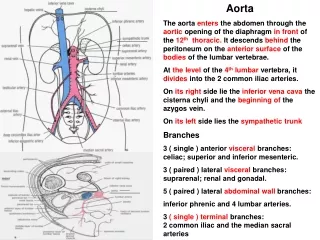
Thoracic Aorta • Anatomy • Ascending aorta • Aortic root & sinuses of Valsalva • Aortic arch • Great vessels: brachiocephalic, left common carotid, & left subclavian arteries • Descending aorta • Intercostal arteries • Anterior spinal artery • Abdominal aorta begins below diaphragm
Thoracic Aorta • Histology • Intima • Media • Adventitia • Physiology • Systole elastic stretch potential energy • Diastole elastic recoil kinetic energy
Aortic Aneurysm • Pathologic dilatation > 1.5 times the normal diameter • Fusiform = symmetric dilatation • Saccular = asymmetric outpoutching • False = contained rupture • Thoracic much less common than abdominal • AAA = 36.5 per 100,000 person-years • TAA = 5.9 per 100,000 person-years
Marfan syndrome AA & arch Ehlers-Danlos syndrome AA & arch Cystic medial degeneration AA & arch Atherosclerosis DA Traumatic Proximal DA Inflammatory Variable Infectious AA (syphilis) Variable (mycotic) Poststenotic AA (aortic stenosis) DA (coarctation) Postsurgical AA (s/p AVR) Etiology
Clinical Course • Natural history & progression of TAA not as well defined as AAA • Onset of symptoms heralds a more rapid course • Dichotomous growth rate • TAAs < 5.0 cm grow 0.17 cm/year • TAAs ≥ 5.0 cm grow 0.79 cm/year • 5-year survival = 20-50% • Rupture is most common cause of death
Clinical Presentation • Vascular complications • AR, CHF, ischemia from compression of coronary artery, sinus of Valsalva rupture into RA or RV with LR shunt, thromboembolism • Compression of external structures • SVC syndrome, dysphagia, hoarseness, respiratory complaints, chest or back pain • Rupture • Sudden, severe, sharp chest or back pain • Left pleural space > pericardium > esophagus
Physical Exam • Diastolic murmur of AR • Signs of CHF • Pulsatile mass in suprasternal notch • Differential pulses in extremities • Signs of SVC syndrome • Decreased air movement or stridor
Diagnosis • CXR – shows widened mediastinum • CT – defines size & extent • MRA – also defines size & extent • TTE – limited use • TEE – role is under evaluation • Aortography – reserved for pre-op eval
Therapy • Medical • β-blockers decrease dP/dT (sheer stress) • Percutaneous • Stent graft for DA distal to left subclavian a. • Surgical • Recommended when maximal diameter is greater than 6 cm • 7 cm for high-risk patients • 5.5 cm for Marfan patients
Surgery • Dacron tube graft • Bentall procedure = valve + graft • Survival • Perioperative mortality = 5-10% • 1-year survival ≥ 70% • 5-year survival = 50-60% • Complications • MI (7.2%), CVA (4.8%), ARF (2.4%), hemorrhage (7.2%), & paraplegia (6.0%)
Gadolinium-enhanced, three-dimensional MRA showing an aneurysm of the aortic arch (arrow) as well as a concomitant atherosclerotic ulcer (arrowhead) Krinsky G et al. N Engl J Med 1997;337:1475-1476
An 84-year-old man with a history of gastric cancer and hypertension was admitted to the emergency department in shock after loss of consciousness Kawasaki S and Kawasaki T. N Engl J Med 2007;356:1251
Aneurysm of Sinus of Valsalva • Results from absence of media • Typically does not cause symptoms • Can compress adjacent structures • Can rupture into adjacent structures • Most commonly into RA or RV • Ventricular septum • Surgical repair typically recommended • Even in asymptomatic patients
Atherosclerosis • Common finding in elderly patients • Aortic plaques are more common in descending aorta > aortic arch > ascending aorta • Typically are irregularly-shaped & frequently are mobile • Can be flow-limiting or hemodynamically-compromising
Atherosclerosis • Independent predictor of long-term neurologic morbitity & mortality • In one study, ulcerated plaque present in 26% of patients with CVA but only 5% of patients without CVA • Plaques > 4 mm thick are more likely to cause an embolic event
Transverse epiaortic ultrasonographic image of the ascending aorta in a patient with severe atherosclerosis of the ascending aorta Kouchoukos N and Dougenis D. N Engl J Med 1997;336:1876-1889
Aortic Dissection • Incidence = 2,000 cases per year in US • 2-to-1 male-to-female ratio • Peak incidence in 6th & 7th decade of life • 65% occur in AA, 20% in DA, 10% in arch, & 5% in abdominal aorta • Mortality (75-80%) is greatest during acute phase (< 2 weeks)
Clinical Presentation • Sudden, severe chest and/or back pain • Tearing, stabbing, or ripping • Less common presentations • CHF (due to AR) • Syncope (due to tamponade) • CVA • Paraplegia • Cardiac arrest
Physical Exam • Hypertension • Hypotension • Pseudohypotension • Diastolic murmur of AR • Signs of CHF • Pulse deficits • Neurologic deficits
Diagnosis • CXR • Widened aortic silhouette • Calcium sign = displacement of intimal calcium > 1 cm from outer aortic soft tissue • CTA • Sensitivity = 83-94% • Specificity = 87-100% • MRA • Gold standard • Sensitivity & specificity ~ 98%
Diagnosis • TTE • Better for AA than DA • Sensitivity = 59-85% • Speficificty = 63-96% • TEE • Sensitivity = 98-99% • Specificity = 77-97% • Depends on experience of operator
CT Scan Showing Localized Dissection of the Aortic Arch with an Intimal Tear (Arrows) Pasic M et al. N Engl J Med 1999;341:1775
MRI of type B aortic dissection Kouchoukos N and Dougenis D. N Engl J Med 1997;336:1876-1889
A 68-year-old woman was admitted to the emergency room with sudden left hemiparesis Pineiro D and Bellido C. N Engl J Med 1999;340:1553
TEE of type A aortic dissection O'Gara P et al. N Engl J Med 2004;350:1666-1674