Download
1 / 30
480 likes | 1.66k Vues
COARCTATION OF AORTA. PRESENTED BY:- AYESHA SULEMAN & BUSHRA HASSAN. CASE PRESENTATION. A 32 year old lady presented to JHL with history of dyspnea on exertion. On examination, her upper extremitities showed. HTN with BP 180/85. femoral pulse was very weak.

E N D
COARCTATION OF AORTA PRESENTED BY:- AYESHA SULEMAN & BUSHRA HASSAN
CASE PRESENTATION • A 32 year old lady presented to JHL with history of dyspnea on exertion. On examination, her upper extremitities showed
HTN with BP 180/85. • femoral pulse was very weak. • Lower extremities showed hypotension. • There was a marked radiofemoral delay. • Inter scapular region showed visible pulsations. • CXR showed cardiac hypertrophy
And the undersurface of the ribs showed notching. MRI showed narrowing of the aorta at the beginning of the descending aorta.
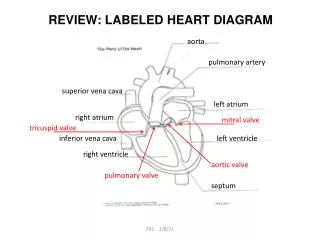
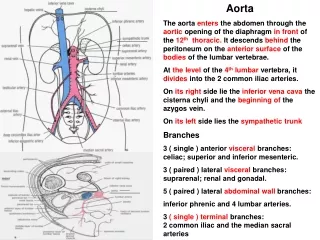
DEFINITION:- • Coarctation of the aorta, or aortic coarctation, is a congenital condition whereby the aorta narrows in the area where the ductus arteriosus (ligamentum arteriosum after regression) inserts.
DUCTUS ARTERIOSUS • In the developing fetus, the ductus arteriosus is a shunt connecting the pulmonary artey to the aortic arch. It allows most of the blood from the right ventricle to bypass the fetus' fluid-filled lungs, protecting the lungs from being overworked and allowing the left ventricle to strengthen.
INTRODUCTION • Coarctation of the aorta (CoA) is a relatively common defect that accounts for 5-8% of all congenital heart defects. Coarctation of the aorta may occur as an isolated defect or in association with various other lesions, most commonly bicuspid aortic valve and ventricular septal defect (VSD). The diagnosis of coarctation of the aorta may be missed unless an index of suspicion is maintained, and diagnosis is often delayed until the patient develops congestive heart failure (CHF), which is common in infants, or hypertension, which is common in older children.
FORMS • There are 2 forms of coarctation of aorta:- • 1. Infantile( with patent ductus arteriosus): It is with tubular hypoplasia of the aortic arch proximal to a patent ductus arteriosus that is often symptomatic in early childhood.
2.Adult hypoplasia: in which there is a discrete ridge like infolding of aorta, just opposite the closed DA distal to the arch vessels.
PATHOPHYSIOLOGY • The vascular malformation responsible for coarctation is a defect in the vessel media, giving rise to a prominent posterior infolding (the "posterior shelf"), which may extend around the entire circumference of the aorta. The gross pathology of coarctation varies considerably. The lesion is often discrete but may be long, segmental, or tortuous in nature
ETIOLOGY • Genetics: Coarctation is 7 times more common in white persons than Asian persons. • Environment: Environmental variation and seasonal variation have been suggested to influence the development of coarctation. A study has shown increased incidence of coarctation in late fall and winter births.
CLINICAL MANIFESTATIONS • Coarctation with PDA usually leads to manifestations in early life usually immediately after birth (poor feeding, tachypnea, letahragy n progress to over CHF n shock. Many infants don’t survive the neonatal period without surgical or catheter based intervention
The outlook is different with coarctation of the aorta without PDA. It is usually symptomatic in adult life. There is HTN in the upper extremities, weak pulses n hypotension in the lower extremities, ass with manifestations of arterial insufficiency( claudication n coldness). Murmurs are presents throughout the systole, a thrill may be present
FREQUENCY • Mortality/Morbidity • Post autopsy studies suggest that the mortality rate in patients in whom coarctation of the aorta is not surgically repaired is 90% by age 50 years, with a mean age of 35 yrs
Race • No definitive racial differences have been documented in coarctation of the aorta, although it is less common in Asians. • Sex • The male-to-female ratio is 2:1
Age • Generally, patients with coarctation of the aorta present early in life with CHF or later in life with hypertension
CLINICAL DIAGNOSIS • 1. Hypertension in the upper extremities. • 2.Weak pulses and low BP in lower extremities • 3.Radiofemoral delay • 4.Murmurs throughout systole • 5.Pulsations in the inter scapular region
LAB DIAGNOSIS • 1.Chest X-ray.. A chest X-ray may show an enlarged heart or a narrowing in the aorta at the site of the coarctation. • 2.Echocardiogram.. An echocardiogram may detect the location and severity of the aortic coarctation
3.Magnetic resonance imaging (MRI). An MRI of the chest will reveal the location of the coarctation of the aorta and determine whether it affects other blood vessels in the body.
4.Cardiac catheterization. It helps determine the severity of the aortic coarctation.
TREATMENT • Treatment approaches usually consist of:- • 1.Surgery • 2.A procedure called balloon angioplasty
Resection with end-to-end anastomosis. This method involves removing the narrowed segment of the aorta (resection) followed by connecting the two ends of the aorta together (anastomosis). • Patch aortoplasty. Patch aortoplasty is useful if the coarctation involves a long segment of the aorta.
Left subclavian flap angioplasty. A portion of the left subclavian artery, may be used to expand the narrowed area of the artery. • Bypass graft repairThis technique involves bypassing the narrowed area by inserting a plastic tube called a graft between the portions of the aorta.
Balloon angioplasty and stentingBalloon angioplasty is an option for initially treating aortic coarctation or for treating re-narrowing (re-coarctation) that has occurred after surgery. During this procedure, we insert a thin flexible tube (catheter) into an artery in your groin and threads it up through your blood vessels to your heart. An uninflated balloon is placed through the opening of the narrowed aorta. When the balloon is inflated, the aorta widens and blood flows more easily. In some cases, a mesh-covered hollow tube called a stent is inserted to keep the narrowed part of the aorta open.
POSSIBLE COMPLICATIONS Aortic aneurysm Aortic dissection Aortic rupture Premature development of CAD Heart failure Stroke Endocardititis Continued narrowing of the aorta
PROGNOSIS • Coarctation of the aorta can be cured with surgery. Symptoms quickly get better after surgery. • Without treatment, most people die before age 40. For this reason, it is usually recommend that the patient has surgery before age 10. Most of the time, surgery to fix the coarctation is done during infancy. • Narrowing or coarctation of the artery can return after surgery. This is more likely in persons who had surgery as a newborn.
PREVENTION • Prevention • There is no known way to prevent this disorder; however, being aware of the risk may make early diagnosis and treatment possible.