Download
1 / 25
300 likes | 1.2k Vues
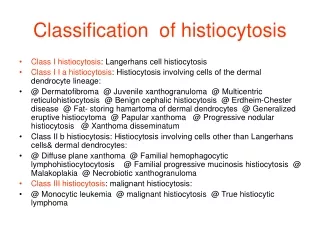
Langerhans Cell Histiocytosis. I2 王鐘慶. Introduction. Accumulation and infiltration of monocytes, macrophages, and dendritic cells in the affected tissues. Classification of Histiocytosis Syndromes in Children. Classification of Histiocytosis.

E N D
Introduction • Accumulation and infiltration of monocytes, macrophages, and dendritic cells in the affected tissues
H&E (left) demonstrates characteristic giant cells (large arrow), eosinophil infiltrate (eosinophil demonstrated between two small arrows), as well as lymphocytes (single small arrow). Positive CD1a immunohistochemistry (right) demonstrates characteristic membranous staining.
EM demonstrating ultrastructural Birbeck granules (cluster between two arrows).
Writing Group of the Histiocyte Society : diagnosis of class I LCH • Presumptive diagnosis - Light morphologic characteristics • Designated diagnosis - Light morphologic features plus 2 or more supplemental positive stains for the following: • Adenosinetriphosphatase • S-100 protein • a-D-Mannosidase • Peanut lectin • Definitive diagnosis - Light morphologic characteristics plus Birbeck granules in the lesional cell with electron microscopy and/or staining positive for CD1a antigen (T6) on the lesional cell
Categories of Langerhans’ Cell Histiocytosis (LCH) • Based on the severity and extent of involvement • Letterer-Siwe disease • Eosinophilic granulomas • Hand-Schuller-Christian disease • Hashimoto-Pritzker disease • Evaluate the extent of involvement and its relationship to prognosis (modified from Egeler and D'Angio classification) • Restricted LCH • Skin lesions without any other site of involvement • Monostotic lesion with or without diabetes insipidus, adjacent lymph node involvement, or rash • Polyostotic lesions involving several bones or more than 2 lesions in one bone, with or without diabetes insipidus, adjacent lymph node involvement, or rash • Extensive LCH • Visceral organ involvement with or without bone lesions, diabetes insipidus, adjacent lymph node involvement, and/or rash but without signs of organ dysfunction of the lungs, liver, or hemopoietic system • Visceral organ involvement with or without bone lesions, diabetes insipidus, adjacent lymph node involvement, and/or rash but with signs of organ dysfunction of the lungs, liver, or hematopoietic system • Location of lesions and extent of the disease have a significant effect on the course of the disease and prognosis
Unifocal LCH (eosinophilic granuloma of bone) • Age: 5-15 years • Solitary calvarial lesion in young adults; other sites of involvement include the vertebra, the rib, the mandible, the femur, the ilium, and the scapula . • Asymptomatic or painful.
Multifocal LCH (Hand-Schuller-Christian disease) • Age: 2-10 years • Fever, diffuse eruption(scalp, ear canal), otitis media, mastoiditis, URI, bone lesions, mild lymphadenopathy, hepatomegaly, and splenomegaly. • Diabetes insipidus (posterior stalk of the hypothalamus) • Hand-Schűller-Christian triad: calvarial bone defects, diabetes insipidus, exophthalmos
Acute disseminated LCH (Letter-Siwe disease) • Age: <2 y/o • Aggressive systemic disorder • fever; anemia; thrombocytopenia; pulmonary infiltrates; skin lesions; and enlargement of the lymph nodes, the spleen, and the liver • Rapid fatal if untreated • With intensive chemotherapy, 5-year survival is about 50%
Clinical Presentation • Bone • Skin • Hypothalamic/Pituitary axis • Other endocrinopathies • CNS • Lymph nodes • Hepatic enlargement • Others
Bone • The most common manifestation (80~100% ) • Skull (27%), femur (13%), mandible/maxilla (11%), pelvis (10%), vertebral bodies (8%), ribs (8%), humerus (5%), and tibia (3%) • The bones of the hands and feet usually spared.
Skin • Up to 50% with multisystem disease may initially present with a rash. • Often the first sign of multisystem LCH • Scaly, erythematous, seborrhea-like brown to red papules, presenting in a fashion similar to contact dermatitis
Hypothalamic/Pituitary axis • Hypothalamic involvement:disturbances in behavior, appetite, temperature regulation, or sleep patterns. • Posterior pituitary involvement: DI
Other endocrinopathies • Growth retardation • Thyroid hormone deficiency • Precocious or delayed puberty, amenorrhea, and hypocortisolism
CNS • Cognitive impairment, emotional lability, changes in behavior, neurologic dysfunction, pyramidal signs, cerebellar symptoms, and cranial nerve palsy (causing difficulties in speech and swallowing) • The most common manifestation is cerebellar symptoms, followed by pyramidal signs and cranial nerve palsy
Lymph node • Lymph nodes are sometimes enlarged in LCH patients (less than 10%), with those from the head and neck region preferentially affected
Hepatic enlargement • Very common in people with disseminated disease (up to 1/3 to 1/2 of children with disseminated disease have hepatomegaly) Signify a later stage of multisystemic disease or a manifestation of a more fulminant disease process
Lung disease • Respiratory distress with tachypnea, retraction, and persistent cough • lung disease is most common in adult LCH patients. • Children with uncontrolled LCH may develop chronic respiratory failure, presenting with cysts or bullae
Others • Otitis • Hypertrophic gingivitis • Oral manifestations may result in bleeding gums, early eruption, or even loss of teeth • GI involvementrare (the most common presenting sign is "failure to thrive" due to malabsorption)
Treatment • Single-agent chemotherapy is the first line therapy.(carboplatin, 2-chlorodeoxyadenosine, chlorambucil, cyclophosphamide, cytosin, arabinoside, daunomycin, etoposide, mercaptopurine, methotrexate, mechlorethamine, procarbazine, vinblastine, vincristine, vindesine) • Topical steroid, intralesional injection of steroids, NSAID, phototherapy, bone marrow allografting, hematopoietic stem cell transplantation, cyclosporin A,prednisoe.