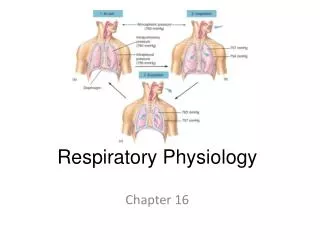
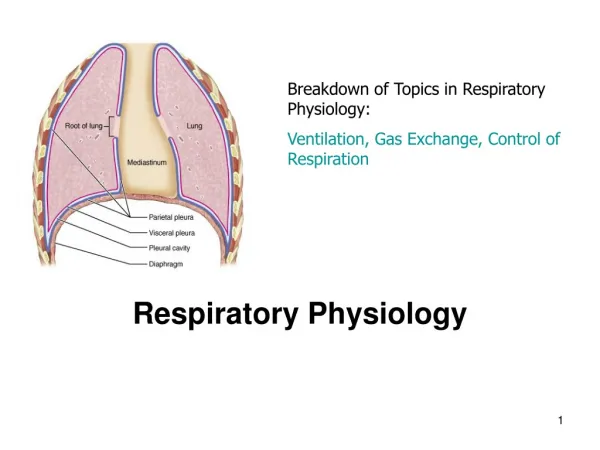
Respiratory Physiology
Respiratory Physiology. Tammy Y Euliano, MD Associate Professor Department of Anesthesiology TEuliano@ufl.edu. Learning Objectives. Clinical assessment of ventilation Differential diagnosis Intervention Supplemental oxygen Mask ventilation Intubation Mechanical ventilation.

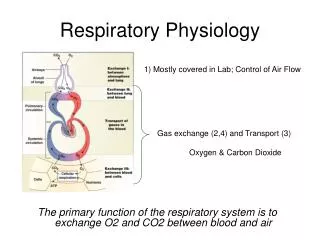
Respiratory Physiology
E N D
Presentation Transcript
Respiratory Physiology Tammy Y Euliano, MD Associate Professor Department of Anesthesiology TEuliano@ufl.edu
Learning Objectives • Clinical assessment of ventilation • Differential diagnosis • Intervention • Supplemental oxygen • Mask ventilation • Intubation • Mechanical ventilation
Case 1: Mr. Block A Medicine patient has become uncommunicative over the last few minutes; he is drooling and cannot open his eyes. He looks “blue.”
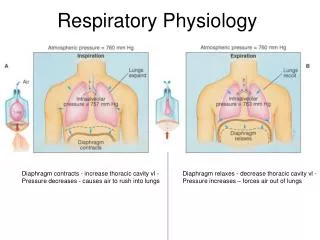
Adequacy of Ventilation • Physical Exam • tachypnea hyperventilation • Measure PETCO2 and/or PaCO2 • Minute Ventilation • MV = VT x RR • Minute Tidal Respiratory • Ventilation Volume Rate • Mechanical(6-10 mL/kg) (8-12 bpm)
Case 1 Summary • Mr. Block received Vecuronium (a paralyzing agent) instead of Vancomycin (an antibiotic) • Supplemental oxygen doesn’t help unless the patient is breathing • Don’t forget the brain may not be asleep in a motionless patient
Case 2: Mr. Poppy One day after a knee operation this otherwise healthy patient has become confused and sleepy.
Alveolar Air Equation PAO2 = PIO2 – (PA CO2 / R) PIO2 = FIO2 x ( PB – PH2O) PIO2 = FIO2 x ( 760 – 47) PAO2 = FIO2 x 713 – (Pa CO2 / 0.8)
Alveolar Air Equation • Room Air PAO2 = 0.21 x 713 – (40/ 0.8) PAO2 = 150 – 50 = 100 • 100% oxygen PAO2 = 1.00 x 713 – (40/ 0.8) PAO2 = 713 – 50 = 663
Case 2 Summary • Mr. Poppy overdosed on opioids resulting in hypoventilation • Supplemental oxygen improves SpO2, but may delay the diagnosis of hypoventilation PAO2 = 0.30 x 713 – (60/ 0.8) PAO2 = 214 – 75 = 139 • Naloxone (Narcan) will reverse opioid-induced hypoventilation, but pay attention to the half-lives of the drugs
Case 3: Mr. Waters A 60 year old man presents to the Emergency Department complaining of shortness-of-breath.
Oxyhemoglobin Dissociation Curve • PaO2 SpO2 • 30 60 • 60 90 • 40 75 • Hypoxia: PaO2 < 60mmHg
Alveolar-Arterial Difference • Alveolar Air Equation to estimate PAO2 • May be approximated as 5 x % Inspired O2 • Compare with PaO2 from ABG, or estimate from SpO2 (saturation by pulse oximeter) • Compare with normal ‘A-a Gradient’ based on patient’s age and the inspired oxygen concentration • Normal PaO2 on Room air is 105 – age/2 • Therefore normal gradient is 5-10 mmHg • Increases with increasing FiO2
Mr. Waters Normal
Compliance Volume / Pressure • Reduced in pulmonary edema, fibrosis, etc • Recognize as increased peak inspiratory pressure
Case 3 Summary • Mr. Waters forgot to take his digoxin and is in congestive heart failure (CHF) with pulmonary edema. • Supplemental oxygen, while indicated, is less effective when the A-a gradient is extremely large due to a diffusion block. • Positive pressure mechanical ventilation may be required.
Case 4: Ms. Match Another Emergency Dept patient complaining of sudden onset of shortness-of-breath and left-sided chest pain.
Dead Space Shunt V/0 0 0/Q Ventilation/Perfusion Mismatch 1 V/Q
Case 4 Summary • Ms. Match suffered a spontaneous pneumothorax • Supplemental oxygen, while indicated, may be ineffective if the A-a gradient is extremely large due to diffusion block or large shunt. • Positive pressure ventilation may worsen a pneumothorax or create a Tension Pneumothorax
Case 5: Mr. Space A post-surgical patient is being weaned from the ventilator. He becomes agitated and the nurse requests an order for sedation.
Hypercapnia • Some things that cause elevated CO2 • Inspiring too much • Making too much • Exhaling too little
Dead Space • Not all gas that moves through the trachea contributes to ventilation VT = VA + VD • Dead Space • Anatomic • Physiologic • Apparatus
Case 5 Summary • Mr. Space was re-breathing CO2 because of an interposed segment of ventilator tubing • Normal anatomic dead space is ~2cc/kg or 150cc