Respiratory Physiology and Function During Anesthesia
510 likes | 1.3k Vues
Explore the three processes of respiration, lung volumes, gas exchange mechanisms, and factors controlling respiration. Learn about ventilation, pulmonary and tissue respiration, and lung capacities. Discover how anesthesia affects respiratory function.

Respiratory Physiology and Function During Anesthesia
E N D
Presentation Transcript
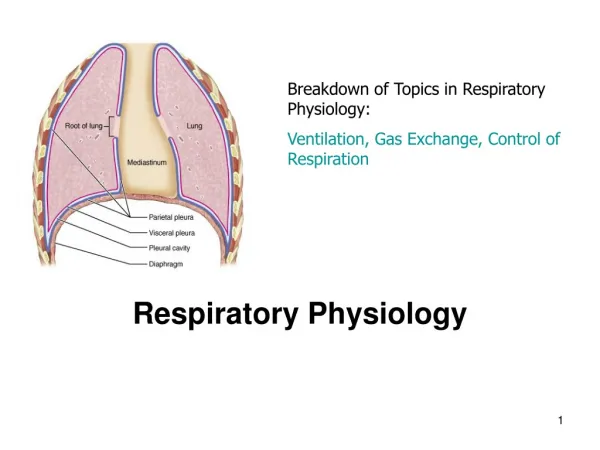
Learning Objectives • Describe the three processes of respiration • Pulmonary ventilation • External respiration • Internal respiration • Identify the various lung volumes and capacities • Describe O2 and CO2 transport • Identify the factors that control respiration • Respiratory Function During Anesthesia
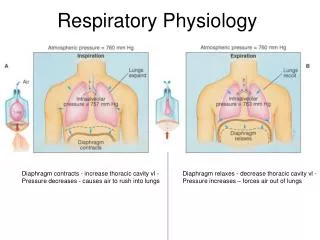
Three Processes of Respiration • Pulmonary ventilation (breathing) • physical movement of air into and out of lungs • inspiration - active • expiration - usually passive • Pulmonary (external) respiration • gas exchange at lung • Tissue (internal) respiration • gas exchange at tissues
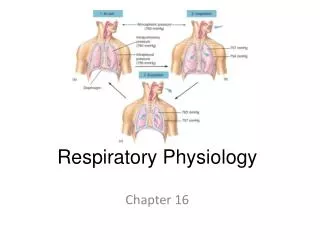
Inhalation • Inhalation • Active process • During quiet breathing contraction of diaphragm and external intercostals expands thoracic cavity • Decreases pressure (Boyle’s law – volume inversely related to pressure) • air flows down pressure gradient
Exhalation • Exhalation during quiet breathing is passive process • Elastic recoil of chest wall and lungs • Due to: • Recoil of elastic fibres • Inward pull of surface tension of alveolar fluid
Deep Forceful Breathing • Deep Inhalation • During deep forceful inhalation accessory muscles of inhalation participate to increase size of thoracic cavity • Sternocleidomastoid – elevate sternum • Scalenes – elevate first two ribs • Pectoralis minor – elevate 3rd–5th ribs • Deep Exhalation • Exhalation during forceful breathing is active process • Muscles of exhalation increase pressure in abdomen and thorax • Abdominals • Internal intercostals
Factors affecting pulmonary ventilation • Surface tension of alveolar fluid • surfactant • Lung compliance • Elasticity • Surface tension • Airway resistance
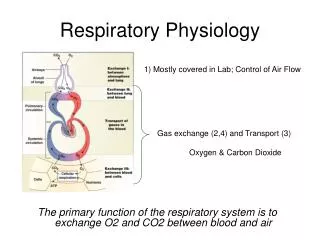
The major task of the lung is: To oxygenate the blood and Eliminate carbon dioxide from it. This is accomplished by exchanging gas between alveoli and pulmonary capillary blood To establish gas exchange in the human lung, there must Be: Ventilation of the alveoli Diffusion through the alveolar-capillary membranes, Circulation or perfusionof the pulmonary capillary bed. The lung is regularly affected by : Anesthesia Mechanical ventilation. Preexisting lung disease Knowledge of the functional impairment : Prevent any disastrous impairment in gas exchange.
Ventilation Dead Space and Alveolar Ventilation Normal tidal breath is approximately 0.5 to 0.6 L Respiratory frequency :16 b/min, Range : 12 to 22breaths/min. Magnitude and rate: Metabolic demand pulmonary function If: Respiratory center is intact and functioning. Ventilation :approximately 7to 8 L/min. VDS: 100 to 150 mL VDS/VT ratio is 0.3 Alveolar ventilation: around 5 L/min . Ventilation-perfusion ratio accordingly is 1.
Increased minute ventilation: Physical exercise, Reduced inspiredoxygen concentration increased dead space ventilation Metabolic acidosis. Increased Dead Space Ventilation If dead space is increased, ventilation must be raised to account for the “losses” and to maintain PaCO2 at anormal level Dead space is increased: Mouthpiece Valve Facemask. “apparatus dead space” : 25 and a few hundred mL, compared 100 to 150 ml (“anatomic dead space”) Bronchiectasis : Vds/Vt ratio = 0.8 to 0.9. mv= 30 to 50 L/min pulmonary embolus (“alveolar dead space”) VDS/VT= 0.7 to 0.8, mv= 20 L/min. Obstructive lung disease, including asthma, chronic bronchitis, and emphysema.
Hyperventilation and Exercise Almost 20-fold higher than resting ventilation, To above 100 L/min in women and above 150 L/min in men, But only for a brief period of half a minute or so. Lower PaCO2 and affect consciousness. Ventilatory capacity perform during rebreathing of expired gas or add CO2 VT to approximately two thirds of vital capacity (VC) , or 2.5 to 4 L Frequency to 40 breaths/min or greater. During maximum physical exercise, minute ventilation increases less, to Two thirds of maximum capacity = 65 to 100 L/min i In athletes, ventilation may exceed 150 L/min.
Lung volumes and capacities • 4 lung volumes: • tidal (~500 ml) • inspiratory reserve (~3100 ml) • expiratory reserve (~1200 ml) • residual (~1200 ml) • 4 lung capacities • inspiratory (~3600 ml) • functional residual (~2400 ml) • vital (~4800 ml) • total lung (~6000 ml)
Lung Volumes Functional Residual Capacity There is a certain amount of air in the lungs after an ordinary expiration. This volume is called functional residual capacity (FRC) Approximately 3 to 4 L , dependent on : Sex Age Height Weigh Exercise Asthma COPD Fibrosis Pulmonectomy The balance of the inward force of the lung and the outward force of the chest wall determines the volume: Inward force of the lung, or “elastic recoil,” Outward force of the chest wall is exerted by the ribs, joints, and muscles
Total Lung Capacity and Subdivisions The gas volume in the lung after a maximum inspiration is called total lung capacity (TLC). It is typically 6 to 8 L COPD increase TLC up to 11 – 12 L RLD deacrease TLC low to 3-4 L Residual volume ~ 2-2.5 L Even after a maximum expiratory effort, some air is left in the lung and no region normally collapses. This persisting gas volume is called residual volume (RV) The maximum volume that can be inspired and expired is called vital capacity. VC is thus the difference between TLC and RV and is around 4 to 6 L. It reduced: Restrictive lung disease Obstructive lung disease.
normal lungs restrictive lungdisease chronic obstructive lung disease
Respiratory Mechanics Understanding the mechanics serves two purposes : 1-what governs the distribution of inspired air. 2- recording as a diagnostic and prognostic tool in lung disease. Compliance of the Respiratory System : The elastic behavior of the lung is often analyzed in terms of compliance, which is the inverse of elastance. Compliance is expressed as change in lung volume divided by the change in pressure required tocause the increment in volume Normal lung compliance is around 0.2 to 0.3 L/cm H2O (2 to 3 L/kPa). It varies with lung volume, and decreases with an increase in lung volume.
Resistance of the Respiratory System Pressure is required to overcome : Resistance to gas flow through the airways during respiration. Sliding of different components of lung tissue and the chest wall. Gas flow : Turbulent - proportional to the square of the pressure Laminar- linearly related to the pressure. Airflow resistance : Normal-1 cm H2O/L/sec. 5 cm H2O/L/sec in mild to moderate asthma and bronchitis Greater than 10 in more severe cases. 8 endotracheal tube - resistance of 5 cm H2O/L/sec Size 7 tube -to 8 cm H2O/L/sec
Distribution of Inspired Gas: Effect of Compliance, Resistance, and Airway Closure
Closing volume (CV) : The volume above RV atwhich airways begin to close during expiration is called closing volume (CV) The sum of RV and CV iscalled closing capacity (CC )
Airflow resistance : Can be higher in expiration than inspiration, Particular forced breathing Patients with obstructive lung disease If resistance is increased during inspiration : probably caused by narrowing of extrathoracic airways Lung tissue resistance : Around 1 cm H2O/L/sec , can be increased threefold to fourfold in chronic lung disease. Chest wall resistance Inertia or Acceleration of Gas and Tissue One additional component of the total impedance to breathing, is inertance, Pressure required to accelerate air and tissue during inspiration and expiration. Is minor under normal breathing More important: Very rapid breathing : HFO, yogi exercise, rapid shallow breathing Can contribute 5% to 10% of the total impedance.
Gas Distribution Distribution of Inspired Gas: Effect of Compliance, Resistance, and Airway Closure During quiet breathing, most gas goes to the lower, dependent regions : increasing lung volume= more and more pressure is required to inflate the lung During inspiration,pleural pressure is lowered, which causes the lower lung regions to inflate more than the upper ones What causes the pleural pressure gradient? Gravity transpulmonary pressure todecrease from the top to the bottom of the lung.
Closing volume (CV) ? The volume above RV at which airways begin to close during expiration Cosing capacity (CC) ? The sum of RV and CV is called closing capacity
Secretions, edema, and spasm affect gas distribution: decreasing or eliminating ventilation Pursed-lips breathing Devices available to breathe out through that act as resistance. Increase in lung volume is the only way of increasin transpulmonary and transairway pressure, and this stabilizes the airway. slow expiratory flow move the EPP up to the larger airways or the mouth, which will prevent floppy airways from collapsing
Diffusion in Airways and Alveoli Total cross-sectional area: Trachea = 2.5 cm2 to: 70 cm2 in the 14th generation entering the acinus 0.8 m2 in the 23rdgeneration. The total alveolar surface is approximately 140 m2. Gas flow velocity will decrease as the area increases: Trachea = around 0.7 m/sec, Alveolar surface it is no higher than 0.001 mm/sec. Transport of O2 and CO2 is therefore accomplished by diffusion in the peripheral airways and in the alveoli, not by convective flow.
Diffusion Across Alveolar-Capillary Membranes • Oxygen diffuses passively from the alveolar gas phase into plasma and red cells, where it binds to hemoglobin. • Carbon dioxide diffuses in the opposite direction, from plasma to the alveoli. • Diffusion over the membranes determined by : • the surface area available for diffusion • (2) the thickness of the membranes • (3) the pressure difference of the gas across the barrier • (4) the molecular weight of the gas, and • (5) the solubility of the gas in the tissues that it has to traverse
Gas Exchange • Exchange of O2 and CO2 between alveolar air and blood occurs via passive diffusion • Governed by • Dalton’s Law • Each gas in a mixture exerts own pressure • Partial pressure • Henry’s Law • Quantity of gas that dissolves in liquid proportional to partial pressure and solubility coefficient • Solubility of CO2 greater than O2 (24x)
External and Internal Respiration • External respiration • Diffusion of: • O2 from alveoli to blood • CO2 from blood to alveoli • Blood leaving pulmonary capillaries mixes with blood draining lung tissue • PO2 of blood in pulmonary veins lower than in pulmonary capillaries • Internal respiration • Diffusion of: • O2 from blood to tissues • CO2 from tissues to blood Jenkins, Kemmitz & Tortora(2007 p. 861)
Pulmonary Perfusion Pressure-Flow Relationship Pulmonary circulation is a low-pressure system. 20 mm Hg systolic and 8 mm Hg diastolic 6 to 10 times lower than systemic Larger vascular diameter , shorter distance =decreases the demand on driving pressur. Pulmonary capillary blood flow is pulsatile Alveolar walls is very thin, without causing any leakage of plasma ,facilitates diffusion of O2 and CO2. ASudden increase pressure to above a mean of 30 mm Hg causes : effusion of plasma into promoting lung edema.
Distribution of Lung Blood Flow A slower increase in pressur=(“vascular remodeling”) : Edema is prevented better, despite even severe pulmonary hypertension,but diffusion capacity will be impaired. Blood flow governed by driving pressure and vascular resistance Gravitational orientation ? playing only a minor role, but there is “fractal” distribution Gravitational Distribution of Blood Flow in the Lung
Nongravitational Inhomogeneity of Blood Flow Distribution
Hypoxic Pulmonary Vasoconstriction HPV : a compensatory mechanism aimed at reducing blood flow in hypoxic lung regions. The major stimulus is low alveolar oxygen tension The stimulus of mixed venous PO2 is much weaker Pulmonary hypertension and pulmonary edema may develop at high altitude Chronic lung disease with hypoxemia also causes HPV, but : Allows time for remodeling of the pulmonary vascular wall: Preventing edema formation
Causes of Hypoxemia and Hypercapnia Causes of hypoxemia classified as : Hypoventilation, V/Q mismatch, Impaired diffusion, Right-to-left shunt. Hypercapnia caused by: Hypoventilation, V/Q mismatch, Shunt In practice hypoventilation is the only cause of real importance
Hypoventilation defined as ventilation that results in a PaCO2 above 45 mm Hg (6 kPa) hypoventilation can be present even when minute ventilation is high : Metabolic demand increased Dead space ventilation is increased Increased alveolar PCO2 reduces the space available for oxygen Thus, PIO2 of 149 mm Hg (19.9 kPa) , PaCO2 of 40 mm Hg (5.3 kPa): PAO2 is 99 mm Hg (13.2 kPa) During hypoventilation ,a PaCO2 60 mm Hg (8 kPa): PAO2 is 74 mm Hg (9.9 kPa)