Download
1 / 1
10 likes | 131 Vues
Impact of Psychiatric Diagnoses on Inpatient Health Care Utilization in Sickle Cell Disease Lisa M. Burks, BA 1 & Matthew P Myrvik PhD 2 , 1 University of Wisconsin-Milwaukee 2 Medical College of Wisconsin Department of Pediatrics, Milwaukee WI. INTRODUCTION. METHODS.

E N D
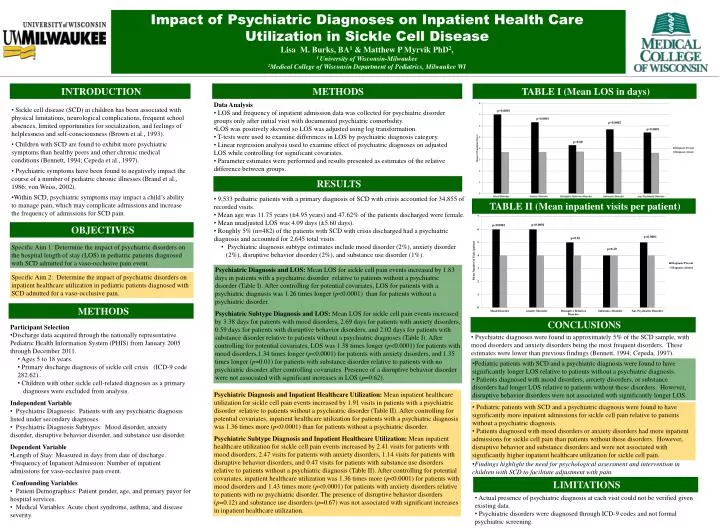
Impact of Psychiatric Diagnoses on Inpatient Health Care Utilization in Sickle Cell Disease Lisa M. Burks, BA1 & Matthew P Myrvik PhD2, 1 University of Wisconsin-Milwaukee 2Medical College of Wisconsin Department of Pediatrics, Milwaukee WI INTRODUCTION METHODS TABLE I (Mean LOS in days) • Data Analysis • LOS and frequency of inpatient admission data was collected for psychiatric disorder groups only after initial visit with documented psychiatric comorbidity. • LOS was positively skewed so LOS was adjusted using log transformation. • T-tests were used to examine differences in LOS by psychiatric diagnosis category. • Linear regression analysis used to examine effect of psychiatric diagnoses on adjusted LOS while controlling for significant covariates. • Parameter estimates were performed and results presented as estimates of the relative difference between groups. • Sickle cell disease (SCD) in children has been associated with physical limitations, neurological complications, frequent school absences, limited opportunities for socialization, and feelings of helplessness and self-consciousness (Brown et al., 1993). • Children with SCD are found to exhibit more psychiatric symptoms than healthy peers and other chronic medical conditions (Bennett, 1994; Cepeda et al., 1997). • Psychiatric symptoms have been found to negatively impact the course of a number of pediatric chronic illnesses (Brand et al., 1986; von Weiss, 2002). • Within SCD, psychiatric symptoms may impact a child’s ability to manage pain, which may complicate admissions and increase the frequency of admissions for SCD pain. RESULTS • 9,533 pediatric patients with a primary diagnosis of SCD with crisis accounted for 34,855 of recorded visits. • Mean age was 11.75 years (±4.95 years) and 47.62% of the patients discharged were female. • Mean unadjusted LOS was 4.09 days (±5.60 days). • Roughly 5% (n=482) of the patients with SCD with crisis discharged had a psychiatric diagnosis and accounted for 2,645 total visits. • Psychiatric diagnosis subtype estimates include mood disorder (2%), anxiety disorder (2%), disruptive behavior disorder (2%), and substance use disorder (1%). TABLE II (Mean inpatient visits per patient) OBJECTIVES p<0.0001 Specific Aim 1: Determine the impact of psychiatric disorders on the hospital length of stay (LOS) in pediatric patients diagnosed with SCD admitted for a vaso-occlusive pain event. Psychiatric Diagnosis and LOS: Mean LOS for sickle cell pain events increased by 1.83 days in patients with a psychiatric disorder relative to patients without a psychiatric disorder (Table I). After controlling for potential covariates, LOS for patients with a psychiatric diagnosis was 1.26 times longer (p<0.0001) than for patients without a psychiatric disorder. Psychiatric Subtype Diagnosis and LOS: Mean LOS for sickle cell pain events increased by 3.38 days for patients with mood disorders, 2.69 days for patients with anxiety disorders, 0.59 days for patients with disruptive behavior disorders, and 2.02 days for patients with substance disorder relative to patients without a psychiatric diagnoses (Table I). After controlling for potential covariates, LOS was 1.38 times longer (p<0.0001) for patients with mood disorders,1.34 times longer (p<0.0001) for patients with anxiety disorders, and 1.35 times longer (p=0.01) for patients with substance disorder relative to patients with no psychiatric disorder after controlling covariates. Presence of a disruptive behavior disorder were not associated with significant increases in LOS (p=0.62). Specific Aim 2: Determine the impact of psychiatric disorders on inpatient healthcare utilization in pediatric patients diagnosed with SCD admitted for a vaso-occlusive pain. METHODS CONCLUSIONS • Participant Selection • Discharge data acquired through the nationally representative Pediatric Health Information System (PHIS) from January 2005 through December 2011. • Ages 5 to 18 years. • Primary discharge diagnosis of sickle cell crisis (ICD-9 code 282.62) . • Children with other sickle cell-related diagnoses as a primary • diagnoses were excluded from analysis. Independent Variable • Psychiatric Diagnosis: Patients with any psychiatric diagnosis listed under secondary diagnoses. • Psychiatric Diagnosis Subtypes: Mood disorder, anxiety disorder, disruptive behavior disorder, and substance use disorder. • Dependent Variable • Length of Stay: Measured in days from date of discharge. • Frequency of Inpatient Admission: Number of inpatient admissions for vaso-occlusive pain event. • Confounding Variables • Patient Demographics: Patient gender, age, and primary payor for hospital services. • Medical Variables: Acute chest syndrome, asthma, and disease severity. • Psychiatric diagnoses were found in approximately 5% of the SCD sample, with mood disorders and anxiety disorders being the most frequent disorders. These estimates were lower than previous findings (Bennett, 1994; Cepeda, 1997). • Pediatric patients with SCD and a psychiatric diagnosis were found to have significantly longer LOS relative to patients without a psychiatric diagnosis. • Patients diagnosed with mood disorders, anxiety disorders, or substance disorders had longer LOS relative to patients without these disorders. However, disruptive behavior disorders were not associated with significantly longer LOS. Psychiatric Diagnosis and Inpatient Healthcare Utilization: Mean inpatient healthcare utilization for sickle cell pain events increased by 1.91 visits in patients with a psychiatric disorder relative to patients without a psychiatric disorder (Table II). After controlling for potential covariates, inpatient healthcare utilization for patients with a psychiatric diagnosis was 1.36 times more (p<0.0001) than for patients without a psychiatric disorder. Psychiatric Subtype Diagnosis and Inpatient Healthcare Utilization: Mean inpatient healthcare utilization for sickle cell pain events increased by 2.41 visits for patients with mood disorders, 2.47 visits for patients with anxiety disorders, 1.14 visits for patients with disruptive behavior disorders, and 0.47 visits for patients with substance use disorders relative to patients without a psychiatric diagnosis (Table II). After controlling for potential covariates, inpatient healthcare utilization was 1.36 times more (p<0.0001) for patients with mood disorders and 1.43 times more (p<0.0001) for patients with anxiety disorders relative to patients with no psychiatric disorder. The presence of disruptive behavior disorders (p=0.12) and substance use disorders (p=0.67) was not associated with significant increases in inpatient healthcare utilization. • Pediatric patients with SCD and a psychiatric diagnosis were found to have significantly more inpatient admissions for sickle cell pain relative to patients without a psychiatric diagnosis. • Patients diagnosed with mood disorders or anxiety disorders had more inpatient admissions for sickle cell pain than patients without these disorders. However, disruptive behavior and substance disorders and were not associated with significantly higher inpatient healthcare utilization for sickle cell pain. • Findings highlight the need for psychological assessment and intervention in children with SCD to facilitate adjustment with pain. LIMITATIONS • Actual presence of psychiatric diagnosis at each visit could not be verified given existing data. • Psychiatric disorders were diagnosed through ICD-9 codes and not formal psychiatric screening.