spinal abscess. why care
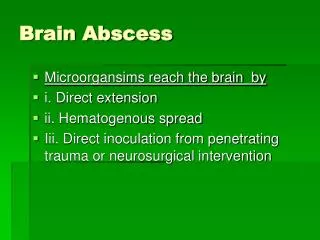
Epidural Abscess. Classic description is focal vertebral pain, which becomes radiating pain along involved nerve roots.Most commonly involves the thoracic spine (50-80% of cases); lumbar in 17-38% and the cervical spine in 10-25% of cases. Spinal epidural abscess most often occurs by systematic hematogenous spread of the infectious organism.A spinal epidural abscess can less commonly occur by direct infection of the epidural space as with a catheter or needle. (eg. Lumbar Puncture).

spinal abscess. why care
E N D
Presentation Transcript
1. Spinal Abscess. Why Care? Irreversible paralysis: affects up to 22% of patients, not because of bacterial virulence but due to delayed diagnosis.*
50% of patients are initially misdiagnosed.**
Paralysis lasting greater than 24 hrs is irreversible.***
6. Predisposing factors Trauma, prior surgery, or spinal procedures.
Immunocompromised states
Pregnancy
Diabetes mellitus (Type I or II)
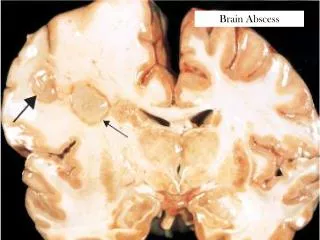
Bacteremia: (endocarditis, lung or abdominal abscess, or previous septic episodes)
Osteomyelitis
IV drug use
Alcoholism
Chronic renal failure
7. Epidemiology 20 patients per 100,000 hospital admissions.
Age < 50 (due to increased prevalence of injection drug users)
Men > Women
8. Buggs 15% in 1996, up to 40% in 200615% in 1996, up to 40% in 2006
9. Diagnosis Classic Triad:
10. Diagnosis Incontinence of bowel/bladder.
Weakness / numbness below the level of the lesion.
12. Diagnosis Nuchal rigidity suggesting the presence of meningeal irritation.
�Four clinical stages of spinal epidural abscess�
onset of focal vertebral pain.
radiation of the pain along regionally involved nerve roots suggesting a radicular component.
evidence of spinal cord compression with long tract signs.
paralysis below the level of the spinal cord lesion.
13. Differential Diagnosis Spinal Radiculopathy / polyradiculopathy
Herniated Disk
Bacterial meningitis.
Osteomyelitis
Spinal tumor / spinal hematoma.
Multiple Sclerosis
Spinal cord infraction (radiating pain along involved nerve roots similar to the pain seen with a spinal abscess. Also, these pts often has sensory impairment and weakness in areas supplied by these roots.)(radiating pain along involved nerve roots similar to the pain seen with a spinal abscess. Also, these pts often has sensory impairment and weakness in areas supplied by these roots.)
14. Pitfalls in diagnosis Stage 2: nerve-root pain radiating from involved spinal area. (no motor weakness or sensory deficit at this point)
Cervical or lumbar abscess: neck pain radiating to the arms or low back pain radiating down to the legs, respectively.
Thoracic abscess: chest or abdominal pain.*
15. Pitfalls in Diagnosis
16. Treatment Neurosurgical consultation for possible decompression.
Empiric antibiotics: Nafcillin or Vancomycin (both for S. aureus) along with Ceftriaxone (Gram-negative) and Metronidazole (anaerobic organisms).
4 weeks course if osteomyelitis is not present.
�and 8 weeks for osteo is present
19. Outcomes