LUNG ABSCESS
LUNG ABSCESS. SIFO ABRAHAM. OUTLINE. DEFINITION CLASSIFICATIONS PATHOPHYSIOLOGY SYMPTOMS PHYSICAL FINDINGS FACTORS CONTRIBUTING TO LUNG ABSCESS DIFFERENTIAL DIAGNOSIS WORKUP TREATMENT. DEFINITION.


LUNG ABSCESS
E N D
Presentation Transcript
LUNG ABSCESS SIFO ABRAHAM
OUTLINE • DEFINITION • CLASSIFICATIONS • PATHOPHYSIOLOGY • SYMPTOMS • PHYSICAL FINDINGS • FACTORS CONTRIBUTING TO LUNG ABSCESS • DIFFERENTIAL DIAGNOSIS • WORKUP • TREATMENT
DEFINITION • Necrosis of pulmonary tissues and formation of necrotic debris containing necrotic debris caused by microbial infection. • The formation of multiple small abscesses <2cm is occasionally referred to as necrotizing pneumonia or lung gangrene.
CLASSIFICATION • Lung abscess is classified based on its duration or etiology. • Acute abscess occuring less than 4-6weeks • Chronic abscess longer duration • Primary abscess caused by aspiration or pneumonia • Secondary abscess caused by obstruction, bronchietasis, immuno-compromised state
pathophysiology • Lung abscess is a complication of aspiration pneumonia caused by mouth anaerobes. • Also caused by septic emboli to the lungs caused by • Bacteremia • Tricuspid valve endocarditis Anaerobes causing lung abscess • Peptostreptococcus spp. • Bacteroides spp. • Fusobacterium spp. • Microaerophilic streptococci
symptoms • The usual symptoms include fever • cough with sputum production • anorexia • weight loss • night sweats. • Hemoptysis and pleurisy
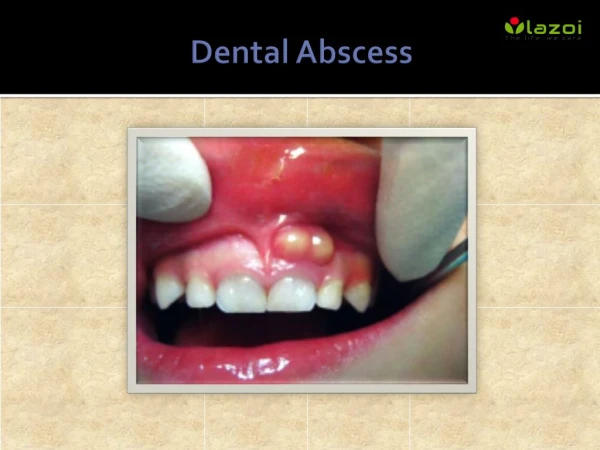
Physical findings • Patients presents with low-grade fever in anaerobic infections & temperature greater than 38.5C in other infections. • Evidence of gingival disease. • Clinical findings of consolidations:{decreased breath sounds, dullness to percussion, bronchial breath sound, course inspiratory crackles
Factors • Oral cavity disease Periodontal disease Gingivitis • Inability to protect airways Alcoholism Coma Drug abuse
Immunocompromised Steroid chemotherapy Malnutrition Multiple trauma • Esophageal disease Achalasia Reflux disease Esophageal obstruction
Bronchial obstruction Tumor Foreign bdy stricture
DIFFERENTIAL DIAGNOSIS • Alcoholism • Empyema, Pleuropulmonary • Hydatid Cysts • Infective Endocarditis • Lung Cancer, Non-Small Cell • Lung Cancer, Oat Cell (Small Cell) • Pneumonia, Bacterial • Pneumonia, Fungal • Pulmonary Embolism • Sarcoidosis • Thrombophlebitis, Septic • Tuberculosis • Wegener Granulomatosis
WORKUPlab studies • CBC • Obtain sputum for gram stain, culture and sensitivity • Blood culture • Sputum for ova and parasite
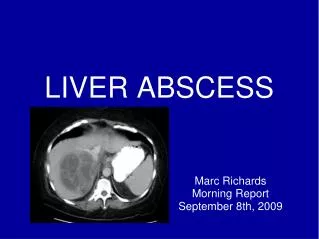
Imaging studies • CXR A typical chest radiographic appearance of a lung abscess is an irregularly shaped cavity with an air-fluid level inside. Lung abscesses as a result of aspiration most frequently occur in the posterior segments of the upper lobes or the superior segments of the lower lobes.
Pneumococcal pneumonia complicated by lung necrosis and abscess formation.
CT scan • CT scanning of the lungs may help visualize the anatomy better than chest radiography. CT scanning is very useful in the identification of concomitant empyema or lung infarction.
TREATMENTantibiotic therapy • Clindamycin: an effective drug over penicillin because several drugs produce beta lactamase thereby showing drug resistance • Metronidazole: an effective drug with a failure rate of 50%
SURGICAL CARE • Surgery is very rarely required for patients with uncomplicated lung abscesses. The usual indications for surgery are failure to respond to medical management, suspected neoplasm, or congenital lung malformation. The surgical procedure performed is either lobectomy or pneumonectomy.
REFERENCES • http://emedicine.medscape.com/article/299425- • http://www.healthline.com/health/lung-abscess#Overview • http://www.patient.co.uk/doctor/lung-abscess