Brain abscess
Brain abscess. * Cause: pyogenic bacteria especially staph . * Routes of infection: Blood-born infection: From acute bacterial endocarditis, lung abscess and bronchiectasis.

Brain abscess
E N D
Presentation Transcript
* Cause:pyogenic bacteria especially staph. * Routes of infection: • Blood-born infection: From acute bacterial endocarditis, lung abscess and bronchiectasis. • Direct spread from adjacent sites: Otitis media, mastoiditis, sinusitis or superior sagital sinus thrombophlebitis.. • Direct inoculation of the bacteria: Compound fractures of the skull.
* The symptoms of brain abscess: • Symptoms of increased intracranial pressure due to a space-occupying lesion (headache, vomiting, confusion, coma), • Symptoms of infection (fever, fatigue etc.) • Focal neurologic brain tissue damage (hemiparesis, aphasia etc.). • The most frequent presenting symptoms are headache, drowsiness, confusion, seizures, hemiparesis or speech difficulties together with fever with a rapidly progressive course.
The symptoms and findings depend largely on the specific location of the abscess in the brain. An abscess in the cerebellum, for instance, may cause additional complaints as a result of brain stem compression and hydrocephalus. • Neurological examination may reveal a stiff neck in occasional cases (erroneously suggesting meningitis). • The famous triad of fever, headache and focal neurologic findings are highly suggestive of brain abscess.
* Diagnosis: • MRI and CT examination. • Note: Lumbar puncture procedure, which is performed in many infectious disorders of the central nervous system is contraindicated in this condition (as it is in all space-occupying lesions of the brain) because removing a certain portion of the cerebrospinal fluid may alter the concrete intracranial pressure balances and causes the brain tissue to move across structures within the skull (brain herniation).
* Morphological features: • Sites: a. If blood born: cerebral at junction between grey and white matter. b. If direct extension: • From otitis media: temporal abscess. • From mastoiditis: cerebellar abscess • From nasal sinuses: frontal abscess.
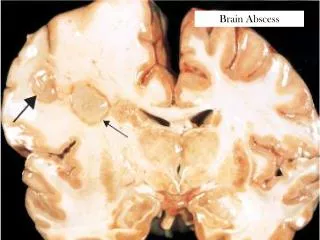
Gross picture: Usually solitary but may be multiple if blood born (pyaemic).
This is a cerebral abscess. There is a liquefactive center with yellow pus surrounded by a thin wall.
* Complication: 1. Direct spread: suppurative encephalitis, subdural abscess, extradural abscess & sinus thrombophlebitis. 2. Rupture into ventricular system (ventriculitis) or subarachnoid space (meningitis). 3. Act as space occupying lesion causing: • Increased intracranial tension: headache, vomiting & papilloedema. • Cranial nerve paralysis. • Hydrocephalus. • Brain herniation.
* Treatment: • The treatment includes lowering the increased intracranial pressure and starting intravenous antibiotics (and meanwhile identifying the causative organism mainly by blood culture studies). • Surgical drainage of the abscess remains part of the standard management of bacterial brain abscesses. The location and treatment of the primary lesion also crucial, as is the removal of any foreign material (bone, dirt, bullets, and so forth).
There are few exceptions to this rule: Haemophilusinfluenzae meningitis is often associated with subdural effusions that are mistaken for subdural empyemas. These effusions resolve with antibiotics and require no surgical treatment. • Tuberculosis can produce brain abscesses that look identical to conventional bacterial abscesses on CT imaging. Surgical drainage or aspiration is often necessary to identify Mycobacterium tuberculosis, but once the diagnosis is made no further surgical intervention is necessary.
* Prognosis: • It was once fatal before the CT era, now, if the abscess is treated before the person goes into a coma. • The death rate has been estimated from 5% to 20% although it is greater in cases of multiple abscesses and when raised intracranial pressure is observed.
Early treatment and the patients overall health has an effect on prognosis. Other factors include: antibiotic resistance or the abscess location. An abscess deep within the brain is more difficult to treat than others.