Pyogenic liver abscess
Pyogenic liver abscess. Suhail Allaqaband Sinai Samaritan Medical Center Milwaukee, WI. The majority of intraabdominal abscesses are not localized to an organ, when a visceral abscess occurs, the liver is most commony involved

Pyogenic liver abscess
E N D
Presentation Transcript
Pyogenic liver abscess Suhail Allaqaband Sinai Samaritan Medical Center Milwaukee, WI
The majority of intraabdominal abscesses are not localized to an organ, when a visceral abscess occurs, the liver is most commony involved • In the best known case series, 540 cases of intraabdominal abscess were identified during a 12-year period • Visceral abscesses accounted for 26 percent • Liver abscesses were the most common visceral abscesses (48 percent) Altemeier, WA, Culbertson, WR, Fullen, WD, Shook, CD. Intra-abdominal abscesses. Am J Surg 1973; 125:70
More recently, 233 cases of liver abscess were reviewed at Johns Hopkins University from 1952 to 1993 • The incidence of liver abscess increased in the years 1973 to 1993 compared to the earlier time period 1952 to 1972 (20 cases per 100,000 admissions versus 13 per 100,000) • A biliary source for the liver abscess was most common • In the earlier time period 28 percent of patients had benign biliary disease, whereas 42 percent had a malignant obstruction in the later years
PATHOGENESIS • The two major mechanisms for the development of liver abscesses are • local spread from contiguous infections within the peritoneal cavity or • hematogenous seeding of the liver • Of the intraabdominal processes, appendicitis with rupture was the most common route for formation of liver abscess in the past • However, as noted above, biliary tract pathology is now the most common cause of liver abscess
Suppurative pylephlebitis, which usually arises from infection in the female genital tract but may result from infection elsewhere in the peritoneal cavity, is another frequent source for bacterial seeding of the liver • Hematogenous seeding is not the usual pathway for the development of liver abscesses in contrast to splenic abscesses which occur less frequently but most commonly arise from bacteremic spread
MICROBIOLOGY • The organisms recovered from liver abscesses are varied and often reflect the origin of the infectious process • Mixed facultative and anaerobic species are isolated most frequently • Approximately 25 percent of cultures of abscess contents contained anaerobes in the Johns Hopkins series • When the biliary tree is the source of infection, enteric gram-negative aerobic bacilli and enterococci are common isolates
MICROBIOLOGY • In liver abscesses arising from pelvic and other intraperitoneal sources, the organisms found in abscess contents are mixed flora including aerobic and anaerobic species (especially B. fragilis) • With hematogenous spread of infection, a single organism is most commonly isolated including S. aureus or a streptococcal species
Many other species of organisms are reported from liver abscesses which reflect geographic differences in prevalence of certain diseases such as Entamoeba histolytica infection as well as common medical interventions including chemotherapy for malignancy and stenting of the biliary tree • Hepatosplenic candidiasis usually presents in patients who have received chemotherapy as neutrophils rebound after a neutropenic episode • Sixty percent of liver abscesses in patients who underwent transarterial embolization for hepatocellular carcinoma in one series were caused predominantly by gram positive organisms
Amoebic liver abscesses are important to consider in patients who are from or have traveled to an endemic area within the past six months • The clinical course and appearance may be indistinguishable from pyogenic liver abscesses • However, amoebic serology is positive in more than 95 percent of cases • Diagnostic aspiration of a suspected amoebic abscess can be required to exclude a pyogenic process, but it is uncommon to find parasites in the abscess contents • Unlike for pyogenic abscesses, drainage of an amoebic liver abscess is not necessary
CLINICALMANIFESTATIONS • The clinical symptoms and signs can be rather protean in liver abscess; the majority of patients do not have symptoms directly referable to the right upper quadrant • Fever is the most common symptom at presentation and occurs in approximately 90 percent of patients • Nonspecific symptoms include • Chills • Anorexia • Weight loss • Nausea and vomiting • Weakness and malaise
Patients, particularly those with active disease of the biliary tract, can have symptoms and signs localized to the right upper quadrant, including pain, guarding, punch tenderness, and even rebound tenderness • However, the absence of right upper quadrant findings on physical examination does not exclude a liver abscess • Only approximately 50 percent of patients with liver abscesses have hepatomegaly, right upper quadrant tenderness, or jaundice
Fever of unknown origin, especially in elderly patients, may be the presenting complaint • Thus, diagnostic studies of the right upper quadrant and the abdomen are important in the evaluation of any patient with an FUO
Liver Abscess and Inflammatory bowel disease • Diseases of the liver and biliary tract are common extraintestinal manifestations of inflammatory bowel disease • Liver abscesses related to Crohn's disease primarily occur in individuals with a known history of IBD, although they can be the initial manifestation of Crohn's disease • Patients present with fever, with or without abdominal pain, jaundice, diarrhea or hepatomegaly
Liver Abscess and Inflammatory bowel disease • The mechanism of abscess formation is unclear • It may be due to direct extension of intraabdominal abscesses or possibly due to portal pyemia with secondary seeding in the liver parenchyma • Successful management requires both drainage of the liver abscess and treatment of the underlying Crohn's disease
Laboratory abnormalities • An elevated serum alkaline phosphatase level is the single most reliable laboratory abnormality • Other tests of liver function may be normal, but 50 percent of patients exhibit elevated bilirubin and 48 percent elevated levels of serum AST • Other laboratory findings include: leukocytosis, normochromic, normocytic anemia, and hypoalbuminemia • Occasionally a chest radiograph can show a new elevation of the right hemidiaphragm, a right basilar infiltrate, or a unilateral pleural effusion
DIAGNOSIS • Scanning techniques are usually required to make a diagnosis of liver abscess • Ultrasonography and CT are the usual diagnostic methods of choice • Gallium or indium-labeled white blood cell scans and MRI can also be used for diagnosis • Gallium or indium scans direct attention to the liver but will not reliably distinguish an abscess from malignancy
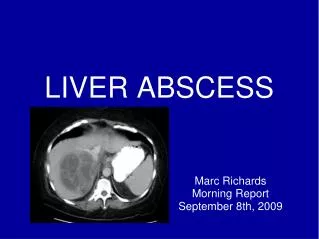
Liver abscess A contrast-enhanced CT scan of the upper abdomen demonstrates a large gas-containing abscess in the right lobe of the liver. This location is easily amenable to percutaneous CT-guided drainage.
TREATMENT • Drainage and antibiotic therapy are important dual treatments for liver abscess
Drainage • Percutaneous drainage has virtually replaced open surgical drainage in the treatment of liver abscess • However, when the two modalities were directly compared in 39 patients, the average length of hospital stay for the percutaneous drainage group was almost double that for open surgical drainage (46 versus 26 days) • Both the time required for fever to resolve and mortality were the same for the two groups • Mortality was considerable, averaging 15 percent, despite treatment Treatment of pyogenic hepatic abscesses: Surgical vs percutaneous drainage. Arch Surg 1986; 121:554
Several factors assist in predicting the failure of percutaneous drainage including • The presence of multiple, sizable abscesses • Viscous abscess contents which tend to plug the catheter • Associated disease (eg, of the biliary tract) that requires primary correction • Direct surgical intervention may be more suitable as a first modality in these situations • Surgery also should be considered when there appears to be no clinical response to percutaneous drainage in 4 to 7 days
Antibiotics • The choice of empiric antibiotic therapy in liver abscess depends upon the probable original source of infection • When an intraabdominal source is suspected, there are a number of antibiotic combinations which can be used • If the biliary tree is the suspected source, the combination of ampicillin (2 gm q 4h IV) and gentamicin, a regimen which covers both Gram negative bacilli, commonly found in infected bile, as well as Enterococcus, is recommended
If a colonic or other intraabdominal site besides the gallbladder is probable, antibiotics should cover both Gram negative bacilli and anaerobes • Aminoglycosides and second- and third-generation cephalosporins are the agents most widely used to cover Gram negative bacilli recovered in intraabdominal processes • Newer antibiotics such as aztreonam, imipenem, piperacillin-tazobactam, ticarcillin-clavulanate, and quinolones (eg, ciprofloxacin) provide excellent coverage of Gram negative bacilli as well, but at a higher cost
The most active and cost-effective antibiotic for anaerobic coverage currently is metronidazole • Other traditional first-line agents include cefoxitin and clindamycin • Gentamicin plus metronidazole is recommended as the initial choice for liver abscess with a probable intraabdominal source
The duration of antibiotic therapy for pyogenic liver abscess is usually long • In general, treatment should be continued until the CT scan shows complete resolution of the abscess cavity • This often requires weeks to months of therapy • In some cases, complete resolution will not occur and antibiotics can be stopped when two CT scans separated by several weeks show no change • When this occurs, patients should be followed carefully for return of fever and an additional CT scan should be performed several months after the last one