Download
1 / 35
350 likes | 709 Vues
IKZ 12 november 2009. Novel developments Radiofrequency Ablation (RFA) for dysplastic Barrett’s esophagus. Erik Schoon, MDL-arts. Barrett’s esophagus. Squamous epithelium displaced by columnar epithelium, containing intestinal metaplasia in the distal esophagus

E N D
IKZ 12 november 2009 Novel developmentsRadiofrequency Ablation (RFA) for dysplasticBarrett’s esophagus Erik Schoon, MDL-arts
Barrett’s esophagus • Squamous epithelium displaced by columnar epithelium, containing intestinal metaplasia in the distal esophagus • Complication of longstanding reflux • prevalence of BE in 10-20% pts with chronic GERD • Swedish general population (n=1000) • - prevalence BE 1.6% • Ronkainen et al, Gastroenterology 2005
Barrett’s esophagus • Premalignant • Adenocarcinoma in BE: • -lifetime risk of 3-5% • annual incidence 0.5% • Malignancy with the fastest rising incidence in the Western world Shaheen et al, Gastroenterology 2000 Devasa et al, Cancer 1998
Intestinal metaplasia Low-grade intraepithelial neoplasia (LGIN) High-grade intraepithelial neoplasia(HGIN) Malignant progression Adenocarcinoma: invasive cancer
Malignant progression Degree of dysplasia correlates with risk of developing cancer Cumulative incidence of cancer in BE (n= 327, median FU 2.4 y) Reid et al, Am J Gastroenterology 2000
Surgery vs. Endoscopic Tx Morbidity (30-50%) Mortality (>3%) Reduces quality of life Preserves the esophagus Low morbidity/mortality
Dutch CBO Guideline Histological evaluation of the ER specimen mucosal lesion submucosal lesion surgical resection Endoscopic treatment or follow-up
CASEHistological outcome endoscopic resection • Radically resected T1m3 adenocarcinoma • Low-risk for metastasis However…… • Residual Barrett’s segment still contained diffuse LGIN.
Intestinal metaplasia Low-grade intraepithelial neoplasia (LGIN) High-grade intraepithelial neoplasia(HGIN) Malignant progression Adenocarcinoma: invasive cancer
After ER, residual BE is at risk for malignant progression • Endoscopic resection (ER) in Barrett’s Esophagus (BE) is effective for removal of focal lesions; • But …after ER monotherapy metachronous lesions in 30% May et al, Eur. J. Gastroenterol, 2002 • Residual BE may be eradicated by: • Stepwise radical endoscopic resection (SRER) • Endoscopic ablation: photodynamic therapy (PDT), argon plasma coagulation (APC), radiofrequency ablation (RFA)
Stepwise Radical Endoscopic Resection Pro:Complete removal of all dysplasia and intestinal metaplasia withhistological correlation. Cons: High rate of stricturing,technically difficult procedure.
Endoscopic Ablation Therapy PhotodynamicTherapy Argonplasma coagulation
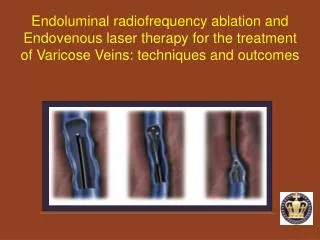
Endoscopic Ablation Therapy Radiofrequency ablation • Pro: • Large areas • Complete removal of BE • No significant side effects • No residual subsquamous IM (“buried Barrett’s”) • Preserves the functional integrity • Removes all genetic alterations • Cons: • Requires multiple treatment sessions
CASEAblation of residual BE mucosa Stepwise circumferential and focal ablation using the HALO system (BÂRRX Corp, Sunnyvale, CA, USA).
Anatomy and RFA Esophageal epithelium ~500µm Lamina Propria Targeted Epithelium Thickness ~500µm Muscularis Mucosae RFA Ablationdepth 500-1,000µm Submucosa Approximate EMR Depth Muscularis Propria
Start sizing 12 cm above TGF Starting too distally can inadvertently measure stomach
Courtesy of Charlie Lightdale, M.D., Columbia Presbyterian, New York
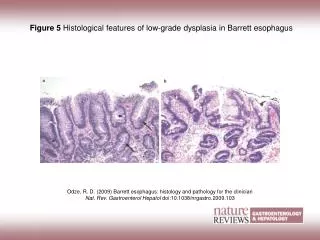
Barrett’s with HGD Biopsy obtained from a columnar-lined esophagus demonstrating HGD [H&E, 400x] Courtesy of John Goldblum, M.D., Cleveland Clinic Foundation
Editorial Clin Gastro 2009 in press • “This approach represents the state-of-the-art in 2009
TREATMENT PROTOCOL HGD/EC in BE ER of any visible lesion Primary HALO360 ablation Residual BE epithelium? YES NO Escape ER EGD with NBI/Lugol and 4Q/1cm biopsies HALO360/90 ablationevery 2 monthsmax. 2x HALO360max. 3x HALO90
Take home message • Endoscopic treatment is treatment of first choice for selected BE patients with HGIN or IMC • ER is the cornerstone of endoscopic treatment and crucial for triage • RF ablation is a promising technique for ablation of Barrett’s neoplasia, that may overcome most drawbacks of current ablation techniques www.rfa-academia.eu