Download
1 / 39
440 likes | 1.09k Vues
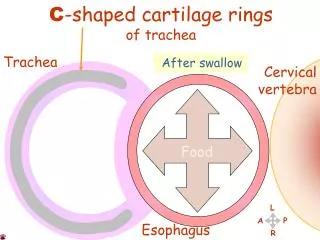
Esophagitis, Barrett Esophagus. Dr M. Abrar Barakzai. Inf. Thyroid Arts. R. Bronch. Art. Thoracic. Aor. Variations: Inf, Phrenic Celiac Splenic Short Gast. Left Gastric Art. Esophagus. Congenital Anomalies Achalasia Hiatal Hernia Diverticula Laceration Varices Reflux

E N D
Esophagitis, Barrett Esophagus Dr M. Abrar Barakzai
Inf. Thyroid Arts. R. Bronch. Art. Thoracic. Aor. Variations: Inf, Phrenic Celiac Splenic Short Gast. Left Gastric Art.
Esophagus • Congenital Anomalies • Achalasia • Hiatal Hernia • Diverticula • Laceration • Varices • Reflux • Esophagitis • Barretts • Neoplasm: Benign, Sq. Cell Ca., Adenoca.
Core symptoms & clinical features • Esophagus • Pain . . . . Heartburn • Nature of the history is important • Big differential • Difficulty in swallowing • History: age and speed of onset • Associated features • Hematemesis - Vomiting of blood that is either fresh bright red, or older "coffee-ground" in character. • Esophegospasm -- Achalasia
Esophagus: congenital and mechanical disorders • Heterotopic tissue(Ectopic tissue) • Usually gastric body type mucosa • Congenitally misplaced • Secrete acid - ulceration and inflammation • Atresia • Failure of canalization in development rate • How might it present? And when? • Diverticula • Traction or pulsion
Congenital Anomalies • Ectopic Tissue (gastric, sebaceous, pancreatic) • Atresia/Fistula/Stenosis/”Webs” • Schatzki“Ring” in lower oesophagus MOST COMMON
Diverticula • Zenker (High) occurs due to increased pressure in the oropharynx during swallowing against a closed upper esophageal sphincter. • Traction (Mid) occur as a consequence of pulling forces on the outside of the esophagus from an adjacent inflammatory process (eg, involvement of inflamed mediastinal lymph nodes in TB). • Epiphrenic (Low) occurs from increased pressure during esophageal propulsive contractions against a closed lower esophageal sphincter. • True Vs. False?
Esophagus: congenital and mechanical disorders • Hiatus hernia • Common - part of the stomach above the diaphragm - dyspepsia • Achalasia • Defective contraction and poor motility • Unknown cause . . Usually reduced ganglion cells • Varices • Secondary to portal hypertension . . . . Serious when they bleed: heamatemesis • Mallory-Weiss tears • Rupture due to severe vomiting . . . .
Hiatal Hernia • Diaphragmatic muscular defect • Widening of the space which the lower oesophagus passes through • In all cases, stomach above diaphragm • Usually associated with reflux • Very common increases with age • Ulceration, bleeding, perforation, strangulation
Achalasia • “Failure to relax” • Aperistalsis • Incomplete relaxation of the LES • Increased LES tone • INCREASE: Gastrin, serotonin, acetylcholine, Prostaglandin F2α, Substance P, histamine, pancreatic polypeptide • DECREASE: Nitric oxide, Vasoactive intestinal polypeptide • Progressive dysphagia starting in teens • Mostly uncertain etiology
Laceration (Mallory-Weiss syndrome) • Tears are longitudinal (lower esophagus) • Usually secondary to severe vomiting • Usually in alcoholics • Usually mucosal tears • By convention, they are all called: • Mallory-Weiss syndrome
Varices • THREE common areas of portal/caval anastomoses • Esophageal • Umbilical • Hemorrhoidal • 100% related to portal hypertension • Found in 90% of cirrhotics • MASSIVE, SUDDEN, FATAL hemorrhage is the most feared consequence
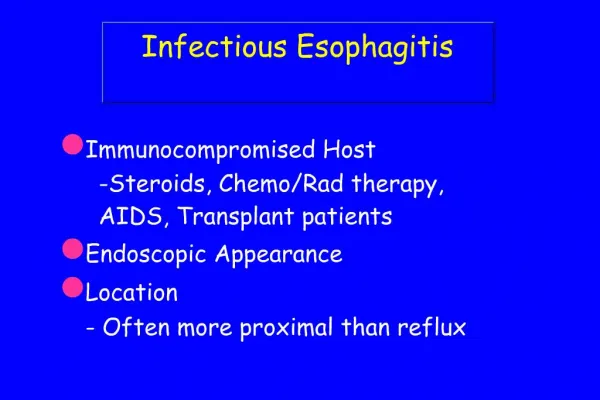
Esophagitis • Acute and Chronic • Chemical • Lye (NaOH,KOH)(suicide attempts) with stricture • Alcohol • Extremely hot drinks • Medicinal pills • Chemotherapy • Infectious • Virus - HSV or CMV, • Fungi - Candida • TB. Crohns disease etc
Reflux Esophagitis GORD/GERD • Gastro oesophageal/esophageal reflux disease • Heartburn • Hiatal hernia • Slow reflex clearing • Poor correlation between symptoms and inflammation • Acid affecting the esophageal mucosa • Defective sphincter mechanisms (LES) • Associated with obesity, smokers etc
Esophagitis - morphology • Increased squamous epithelial turnover • Basal layer hyperplasia • Prominent papillae • Increased desquamation • Inflammation may actually be quite mild • Eosinophils, Neutrophils, Lymphocytes.
Complications of esophagitis • Ulceration • Acute inflammation seen • Bleeding/hematemesis • Scarring/Fibrosis • Stricture formation . . Progressive dysphagia • If prolonged may develop epithelial metaplasia (Barrett’s Esophagus)
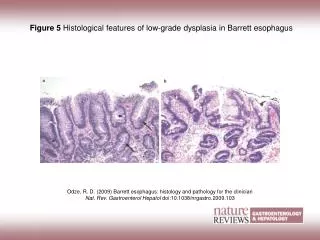
Barrett’s Esophagus • Long term consequence of GERD • Occur in 10% of individuals with symptoms of GERD • Metaplasia of squamous epithelium to a glandular epithelium (columnar lined oesophagus = CLO) • Presence of goblet cells in the esophageal mucosa is diagnostic • Increased risk of adenocarcinoma of the esophagus • Epithelial dysplasia may arise in the areas of metaplasia • Management controversial but endoscopy and biopsy at intervals advised by most authorities
Increasing CLO: true prevalence and increasing recognition Short Segment < 3 cm. And Long segment > 3 cm. Increasing gastro-oesophageal reflux disease Risk factors for reflux disease: male middle age white overweight alcohol smoking family history Epidemiology of Barrett’s oesophagus and its complications
Pathogenesis . . . • Textbooks say squamous epithelium BECOMES glandular . . . • Probably actually an overgrowth of the normal esophageal glands who increase and ‘dominate’ the squamous epithelium. • Additional genetic changes (esp p53 mutation) provide a milieu for dysplasia and eventually malignancy
South West Cancer Registry, 1983-1992 Percent Adenocarcinoma Squamous cell carcinoma 83 84 85 86 87 88 89 90 91 92
‘Importance’ incidence, mortality, morbidity and perception Incidence of Oesophageal Adenocarcinoma in England and Wales 4000 3500 3000 2500 Mortality 2000 1500 1000 500 0 94 79 89 84 97 Year ONS 1999
Predicting who will get tumours Very hard • Why . . ? • Many people have GERD . . . Some have Barretts . . Some get tumours . . • Those with established Barrett have ~ 100x increase in adenocarcinoma . . . • Most people who get Adenocarcinoma were never known to have Barrett’s.