Download
1 / 28
300 likes | 605 Vues
Esophagus cancer. Dr Sanei Associated professor of pathology GI and Liver patholoogist. Pathogenesis. food or water rich in nitrates and nitrosamines tobacco smoke , alcohol , and various vitamin deficiencies achalasia Plummer-Vinson syndrome

E N D
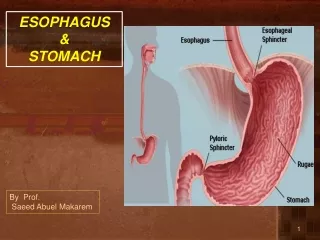
Esophagus cancer Dr Sanei Associated professor of pathology GI and Liver patholoogist
Pathogenesis • food or water rich in nitrates and nitrosamines • tobaccosmoke, alcohol, and various vitamin deficiencies • achalasia • Plummer-Vinson syndrome • strictures resulting from acid or lye ingestion • HPV types 16 and 18. 0% to 66%
Molecular Features • cyclin D1 and cyclin E • p53, Rb, and p16 in up to 80% • epidermal growth factor receptor (EGFR), seen in from 29% to 92%
SQUAMOUS DYSPLASIA • low grade and high grade • 60% to 90% • erythematous, friable, and irregular in more than 80% • Erosions, plaques, and nodules • normal endoscopically • reactive epithelial changesindefinite for dysplasia • chemotherapy or radiotherapy • esophagitis secondary to reflux, or other causes such as drug effect
INVASIVE SQUAMOUS CELL CARCINOMA • early (superficial) and late (advanced) • middle third of the esophagus in 50% to 60% of cases • Superficially invasive tumors are more commonly multicentric up to 20% of cases • fungating (60% of cases), ulcerating (25% of cases), or infiltrative (15% • In patients treated with preoperative radiation or chemotherapy, the tumor may be invisible or perhaps replaced with a shallow surface erosion.
cytokeratins13, 14, 18, and 19.[65], [66] CK7 reactivity is present in up to 29% of cases • majority of cases are negative for both cytokeratins 7 and 20 • most tumors express the nuclear antigen p63 • Focal positivity for neuroendocrine markers such as chromogranin and synaptophysin • Mucin stains may show focal positivity
Differential Diagnosis • lung squamous cell carcinomas thyroid transcription factor F1 (TTF-1), • pseudoepitheliomatous hyperplasia • melanoma • lymphoma • pseudodiverticulosis
ADENOCARCINOMA • More than 95% of esophageal adenocarcinomas develop in association with Barrett's esophagus • Non–Barrett's-Associated Adenocarcinoma • extremely rare and arise either from foci of gastric heterotopia • submucosal gland/duct system • Adenoid Cystic Carcinoma
CARCINOMA WITH MIXED SQUAMOUS AND GLANDULAR ELEMENTS • adenoacanthoma • adenosquamous carcinoma • mucoepidermoid carcinoma
METASTASES • lung, breast, and stomach • renal cell carcinoma