Tracheostomy safety
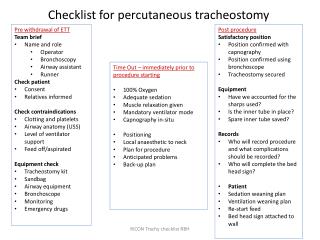
Tracheostomy safety. Lessons from the Coroner’s Court. What I plan to cover. Lessons regarding tracheostomy safety from a single event Update on national learning and initiatives for tracheostomy safety Lessons learnt about going to the coroner. Our patient – pre - ITU stay.

Tracheostomy safety
E N D
Presentation Transcript
Tracheostomy safety Lessons from the Coroner’s Court
What I plan to cover • Lessons regarding tracheostomy safety from a single event • Update on national learning and initiatives for tracheostomy safety • Lessons learnt about going to the coroner
Our patient – pre - ITU stay • 66 year old female • Expressive dysphasia and confusion • Herpes simplex encephalitis plus L tempero-parietal infarction
MRI scan 3 days after admission
Our patient – ITU stay • 66 year old female • Expressive dysphasia and confusion • Herpes simplex encephalitis plus L tempero-parietal infarction • Day 4 after admission, HAP, reduced GCS and needed IPPV • Further complicated by diarrhoea, MRSA in sputum • Day 16 = tracheostomy for weaning done in theatre
HDU stay • HDU step down on day 28 • Slow and incomplete neuro recovery. Interacting a bit, especially with daughter • Day 49, plan made for step down to medical (respiratory) ward on day 52 • Transfer delayed due to diarrhoea outbreak on the ward • Day 53, evening, Friday: sudden need for critical care beds x 2, so stepped down to surgical tracheostomy care ward instead.
Ward stay – why we are here • Decision made at 17:45h Friday • Transfer happened in small hours of Saturday • Over Saturday she removed her NG feeding tube and humidified oxygen mask. • Junior doctor review: subcutaneous fluids prescribed but not put up until 01:00 Sunday • Seen at 07:20h and showed no distress • Found collapsed at 07:45h. 2222 call. Unable to ventilate down tracheostomy tube. • Replaced by oral tube by trainee anaesthetist. Not able to be resuscitated.
Coroner’s summing up • “The provision of a tracheostomy mandated a strictly adhered to regime of management and care. In particular it was necessary to make provision for regular cleaning and suctioning of secretions with the administration of warmed humidified oxygen in a well hydrated patient to avoid secretions becoming overly sticky increasing the risk of a blocked canula.”
Coroner’s perceptionof risk “The cerebral infarction had left the patient totally dependent on the care of medical staff for survival. She could not speak so as to summons help when physically distressed and nor could she muster the coordination or comprehension so as to activate an alarm. As such she was at all times dependent on regular monitoring and anticipation of her needs. Further she was subject to agitation, was known to have a tendency to pull out lines and to have a tendency to build up secretions necessitating regular cleaning of tracheostomy tubing.”
Coroner’s perceptionof risk “The cerebral infarction had left the patient totally dependent on the care of medical staff for survival. She could not speak so as to summons help when physically distressed and nor could she muster the coordination or comprehension so as to activate an alarm. As such she was at all times dependent on regular monitoring and anticipation of her needs.Further she was subject to agitation, was known to have a tendency to pull out lines and to have a tendency to build up secretions necessitating regular cleaning of tracheostomy tubing.”
Coroner’s perceptionof risk “The cerebral infarction had left the patient totally dependent on the care of medical staff for survival. She could not speak so as to summons help when physically distressed and nor could she muster the coordination or comprehension so as to activate an alarm. As such she was at all times dependent on regular monitoring and anticipation of her needs. Further she was subject to agitation, was known to have a tendency to pull out lines and to have a tendency to build up secretions necessitating regular cleaning of tracheostomy tubing.”
Factors contributing to danger • Patient • Total dependence • Tendency to build up secretions • Uncoordinated and unable to communicate her needs • Institutional • Lack of documentation of basic care • Lack of formal training structure • Failure to handle delirium • Failure to stick to plans
What is the risk of a tracheostomy? • Few papers on this and definitions vary • About 1/200 die as a consequence of having a tracheostomy • Heterogeneous group of papers, not all relevant to post-critical care
Familiar problem (2) • 85% of intensivists aware of clinically significant event in ITU performed tracheostomies including • 52% secretions • 52% displacement • 89% discharge to the ward or other step down.
A major problem Postgrad Med J 2010;86:522e525
Major problem (2) • 2 years reports to NPSA • 968 safety reports concerning tracheostomy events on wards • 453 affected patients • 338 harmed patients • 83 = more than temporary harm • 15 deaths in which tracheostomy implicated. Postgrad Med J 2010;86:522e525
NAP 4 Displaced tracheostomy, and to a lesser extent displaced tracheal tubes, were the greatest cause of major morbidity and mortality in ICU. Obese patients were at particular risk of such events and adverse outcome from them. All patients on ICU should have an emergency re-intubation plan.
NAP 4 - ICU planning In ICU planning should recognise that intubation sometimes fails, that tracheal tubes and tracheostomies will inadvertently fall out and that all these events are more likely to occur in obese patients. Tracheal tube and tracheostomy displacement in ICU was repeatedly reported after patient movement or patient interventions and this has been reported before.
National Tracheostomy Safety Project www.tracheostomy.org.uk
1 of 3 www.tracheostomy.org.uk
Going to theCoroner • Meet up beforehand in good time • Use this opportunity to review your safety measures in place at the time • What you have done since, and what you think you should do further before the day? • If you think you are going to have rough time, take big guns • Apologise • Don’t try to deflect blame when you are to blame • Go back to original material, not other people’s summaries • Know your own Trust documents