TRACHEOSTOMY
. Tracheostomy is an operative procedure that creates a surgical airway in the cervical trachea. . Relevant Anatomy . The larynx is composed of 3 large cartilage units: the epiglottis, the thyroid, and the cricoid cartilage. The cricoid cartilage is described as a reverse signet ring just inferior

TRACHEOSTOMY
E N D
Presentation Transcript
1. TRACHEOSTOMY
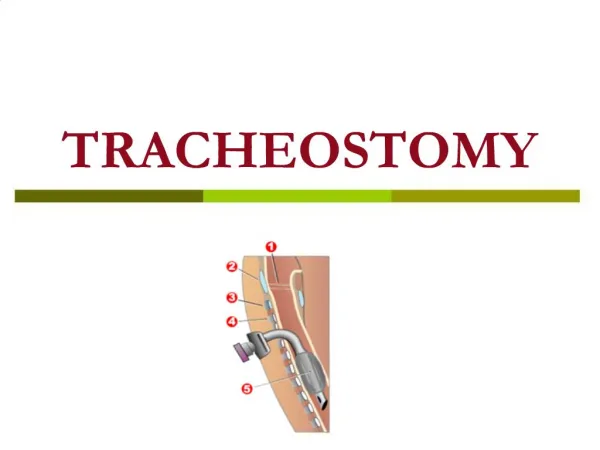
2. Tracheostomy is an operative procedure that creates a surgical airway in the cervical trachea.
3. Relevant Anatomy The larynx is composed of 3 large cartilage units: the epiglottis, the thyroid, and the cricoid cartilage.
The cricoid cartilage is described as a reverse signet ring just inferior to the thyroid cartilage. The cricothyroid membrane stretches between the thyroid and cricoid cartilages.
5. The trachea is membranous posteriorly and is formed of semicircular cartilaginous rings anteriorly and laterally. The spaces between the rings are membranous.
The recurrent laryngeal nerves and inferior thyroid veins that travel in the tracheoesophageal groove are paratracheal structures vulnerable to injury if dissection strays from the midline.
6. The thyroid gland lies anteriorly to the trachea with a lobe on both sides and the isthmus, which crosses the trachea at approximately the level of the second and third tracheal rings.
This tissue is extremely vascular and must be divided with careful hemostasis.
7. INDICATIONS To bypass obstruction
Congenital anomaly (eg, laryngeal hypoplasia, vascular web).
Foreign body that cannot be dislodged with Heimlich and basic cardiac life support (BCLS) maneuvers.
Supraglottic or glottic pathologic condition (eg: infection, neoplasm, bilateral vocal cord paralysis).
8. INDICATIONS Neck trauma that results in severe injury to the thyroid or cricoid cartilages, hyoid bone, or great vessels.
Subcutaneous emphysema.
Facial fractures that may lead to upper airway obstruction (eg: comminuted fractures of the midface and mandible).
To provide a long-term route for mechanical ventilation in cases of respiratory failure.
9. INDICATIONS Prophylaxis (as in preparation for extensive head and neck procedures and the convalescent period).
Severe sleep apnea not amendable to continuous positive airway pressure (CPAP) devices or other, less invasive surgery.
10. INDICATIONS Edema
Trauma
Burns
Infection
Anaphylaxis
11. Contraindications No absolute contraindications exist to tracheostomy.
12. Types of Tracheostomy Emergency: Patients in acute respiratory distress may need acute surgical intervention. This can be performed with the patient under local anesthesia.
Elective:Most elective tracheostomies are performed in patients who are already intubated and who are undergoing a tracheostomy for prolonged intubation. A smaller population of patients with chronic pulmonary problems (eg, sleep apnea) elect to undergo tracheostomy.
Permanent:in case of bilateral abductor palsey or
laryngeal stenosis.
13. Intraoperative details The performance of an open tracheostomy is varied.
The unconscious or anesthetized patient is positioned supine with the neck extended and the shoulders elevated on a small roll.
The awake patient does not tolerate this; therefore, the procedure is performed with the patient in a sitting or semirecumbent position.
14. Intraoperative details Overextension of the neck should be avoided because it further narrows the airway; additionally, overextension can lead to placement of the tracheostomy too low (toward the carina) and too close to the innominate artery (especially in the very mobile pediatric trachea).
Important landmarks (eg, thyroid notch, sternal notch, cricoid cartilage) are palapated, and marked .
A 3-cm vertical incision that extends inferiorly from the cricoid cartilage is planed, and lidocaine (1%) with 1:150,000 parts epinephrine is infitrated.
15. Intraoperative details A vertical incision is made.
Many advocate the horizontal skin incision, which is made along relaxed skin tension lines and gives better cosmesis.
A horizontal incision may trap more secretions.
Meticulous hemostasis is important throughout, beginning with the skin edges.
16. Intraoperative details Subcutaneous fat may be removed with electrocautery to aid in exposure and to prevent later fat necrosis.
Dissection proceeds through the platysma until the midline raphe between the strap muscles is identified.
the inferior limit of the field is palpated to assess the proximity of the innominate artery.
aberrant anterior jugular veins and smaller vessels are cauterized or ligated.
The strap muscles are separated and retracted laterally, exposing the pretracheal fascia and the thyroid isthmus. The lateral retraction also serves to stabilize the trachea in the midline.
17. Intraoperative details the thyroid isthmus, which typically lies anteriorly over the first 2-3 tracheal rings is often divided.
The isthmus is elevated off the trachea with a hemostat and divided it.
The anesthesiologist is warned of impending airway entry.
The endotracheal tube balloon is deflated and entered into the trachea.
Injection of topical anesthesia can stem the cough reflex of an awake patient.
18. Intraoperative details After the trachea is entered, secretions and blood is suctioned out of the lumen and the endotracheal tube is slowly withdrawen to a point just proximal to the opening.
and previously tested tracheostomy tube is inserted.
After the airway is confirmed intact based on carbon dioxide return and bilateral breath sounds, the tracheostomy tube is secured to the skin with 4-0 permanent sutures.
19. Choice of tube Typically, the smallest feasible tube should be used.
A rule is that the tube should be three fourths of the diameter of the trachea.
Cuffed tubes allow positive pressure ventilation and prevent aspiration.
Cuffs should be deflated regularly (qid) to prevent pressure necrosis.
20. Choice of tube Tracheostomy tubes vary in size, degree of arc, and length.
It is consisted of three parts 1.outer cannula 2.obturator 3.inner cannula
21.
The outer cannula fits directly into the tracheal stoma.
Proximal flange designs vary to accommodate mechanisms for securing the tube in place and/or locking the inner cannula.
The distal end of the outer cannula may or may not incorporate a cuff that, when inflated, prevents air leakage between the tracheal wall and outside of the tracheostomy tube. This seal facilitates ventilatory assistance and/or minimizes aspiration.
Tracheostomy tube cannulae may be fenestrated along the greater curvature to allow for air passage through the tube and upward toward the pharynx. Such fenestra are utilized for speech production and/or preparation for decannulation
22.
The obturator is inserted into the outer cannula to facilitate insertion into the trachea.
Because the obturator occludes the lumen of the tracheostomy tube and therefore the patient�s airway, it is immediately removed after the outer cannula is in its proper location.
The obturator should be kept readily available for reinsertion in the event of tracheostomy tube displacement. It should always accompany the patient (eg, to x-ray).
23.
The inner cannula is inserted into the outer cannulae and locked into place. Locking mechanisms vary, and the inner cannula may or may not incorporate a 15 mm adaptor for use with ventilatory equipment (ie, ventilation bag, ventilator tubing). Nondisposable inner cannulae should only be removed for cleaning. Not all types of tracheostomy tubes have inner cannula.
24.
1. Jackson (plain) Tracheostomy Tube: This stainless steel tube does not have a cuff or 15 mm adaptor. Available in sizes 00 through 10.
2. Lorae Tracheostomy Tube: Identical to Jackson tube except that inner cannula has a 15 mm adaptor.
3. Shiley Low Pressure Cuffed Tracheostomy Tube : This cuffed plastic tube has locking inner cannula with 15 mm adaptor. It is available in even sizes 4, 6, 8, and 10.
28. Postoperative details Postoperative care is critical.
The recently insulted trachea produces copious secretions, and irrigation with saline and suctioning every 15 minutes are not initially unreasonable.
Suctioning should be limited to the length of the tube to avoid tracheal ulceration and tracheitis and should be limited to no more than 15 seconds because the act of suctioning blocks the airway and sucks the air out of the lungs.
Humidified oxygen helps prevent inspissation of the secretions. Additional mucolytic agents (eg, acetylcysteine [Mucomyst], guaifenesin) may be used. If uncorrected, mucus that plugs the inner cannula can cause a life-threatening obstruction.
29. The original tube is left sutured in place for 5-7 days to allow the tract to heal.
The sutures are then removed, and the tube is replaced.
For patients in whom the tracheostomy was an acute intervention, this is an opportunity to downsize the tube or to change to a metal (Jackson) tube.
The site should be kept clean and dry to minimize infection from what is a chronically colonized location.
30. Follow-up care Speaking
As soon as the cuff can be deflated, the patient should be encouraged to occlude the tube with a finger and to begin to phonate.
As long as no significant edema is present, enough air passes by the tube and through the vocal cords.
This encourages the patient to reestablish normal airflow through the upper airway and diminishes psychological reliance on the lesser resistance of the tracheostomy.
31. Passy-Muir valves are special 1-way valve caps that allow automatic occlusion with exhalation for speech. Negative pressure (inspiration) opens the valve.
Plugging: In preparation for decannulation, the tracheostomy tube may be plugged. The patient must be able to remove the plug should dyspnea develop. Patients with sleep apnea frequently keep their tubes plugged except when they go to sleep.
Swallowing: Swallowing is more difficult while the tube is in place because of decreased laryngeal elevation; however, oral intake is certainly possible. Thoroughly evaluate the patient's risk of aspiration before feeding begins.
32. Home care and equipment:
Tracheostomy remains socially stigmatized and can intimidate both the patient and the family.
The family's understanding and comfort are most important. Education must begin early, and preparations for discharge must be complete.
The most commonly overlooked or misunderstood item is the obturator, which is important in the a traumatic reinsertion of the outer cannula.
33. COMPLICATIONS Immediate complications
Apnea due to loss of hypoxic respiratory drive: This is mainly important in the awake patient. Ventilatory support must be available.
Bleeding: Intraoperative bleeding arises from the cut edges of the very vascular thyroid gland and from lacerated vessels in the field that should be cauterized or ligated.
Pneumothorax or pneumomediastinum: These can result from direct injury to the pleura or the cupola of the lung (especially in children) or from high negative inspiratory pressures of patients who are awake and distressed. Early recognition is critical, and routine postoperative chest radiography should be considered after tracheotomy.
Injury to adjacent structures: The paratracheal structures vulnerable to injury are the recurrent laryngeal nerves, the great vessels, and the esophagus. This danger is most prevalent in children because the softness of the trachea hinders its identification if it is not distended with a rigid object.
Postobstructive pulmonary edema: Although rare, a transient pulmonary edema can occur after tracheostomy, which provides relief of upper airway obstruction.
34. Early complications
Early bleeding: This is usually the result of increased blood pressure as the patient emerges from anesthesia (and relative hypotension) and begins to cough.
Plugging with mucus: The use of dual cannula tubes lessens this as a threat because the inner cannula can be removed for cleaning while the outer cannula safely maintains patency of the fresh tract. However, vigilance is still required, and all measures to thin and to remove secretions should be undertaken.
Tracheitis: To some degree, tracheitis is present in all patients with fresh tracheostomies. Again, humidification, minimization of the fraction of inspired oxygen (FIO2) (because high oxygen levels exacerbate drying), and irrigation are essential. Moreover, motion of the tube within the trachea is extremely irritating and should be prevented with stabilization of the ventilator circuitry so that torsion is minimized.
Cellulitis:
35. Displacement
The need to replace a new tracheostomy tube is not uncommon. In this situation, remember the access that the upper airway still affords. Bag ventilate the patient and prepare for intubation if the tracheostomy tube cannot be replaced. Initial management includes passing an object (eg, smaller tube, clear nasogastric tube [which shows the fogging of respiration]) into the open wound.
A physician may attempt recannulation. This is facilitated with placement of the tube over the fiberoptic laryngoscope and reentry of the trachea under direct vision. However, endotracheal intubation remains the mainstay of airway management and should not be ignored while an increasingly traumatized tracheostomy site is labored over. Misplacement of the tracheostomy tube into the dreaded false passage, usually in the pretracheal space, should be suspected in the presence of difficult ventilation or passage of a suction catheter or if subcutaneous air or pneumothorax develops.
36. Subcutaneous emphysema: This results from a tight closure of tissue around the tube, tight packing material around the tube, or false passage of the tube into pretracheal tissue. It can progress to pneumothorax, pneumomediastinum, or both and should be treated with loosening of the closure or packing and with performance of a tube thoracotomy, if necessary. Incidence of pneumothorax after tracheostomy is 0-4% in adults and 10-17% in children; thus, postoperative chest radiography is recommended in children.
Atelectasis: An overly long tube can mimic a unilateral mainstem intubation, causing atelectasis or collapse of the opposite lung.
37. Late complications Bleeding
Tracheomalacia
Stenosis
Tracheoesophageal fistula
38. OUTCOME AND PROGNOSIS Duration of tracheostomy: A tracheostomy can be used for days or, with proper care, for years.
Decision to decannulate: The tracheostomy tube should be removed as soon as is feasible and, therefore, should be downsized as quickly as possible. This allows the patient to resume breathing through the upper airway and reduces dependence (psychological and otherwise) on the lesser resistance of the tracheostomy tube. Decannulation may be performed when the patient can tolerate plugging of the tracheostomy tube overnight while asleep without oxygen desaturation. After the tube is removed, the skin edges are taped shut, the patient is encouraged to occlude the defect while speaking or coughing, and the wound should heal within 5-7 days.
39. In an acute emergency, cricothyrotomy secures an airway more rapidly than tracheostomy, with fewer potential immediate complications such as pneumothorax and hemorrhage.
Percutaneous dilatational tracheostomy as an elective bedside (or intensive care unit) procedure has undergone scrutiny in recent years as an alternative to tracheostomy.
Simultaneous videobronchoscopy can reduce the incidence of major complications.
40. 1.Which of the following prevents the aspiration of foods and liquids?
A. Epiglottis
B. Cricoid cartilage
C. Arytenoid cartilages
D. Thyroid cartilages
41.
2.Which part of Larynx K/A Adam�s apple.
A. Epiglottis
B. Cricoid cartilage
C. Arytenoid cartilages
D. Thyroid cartilages
42. Largest cartilage of Larynx?
43. Ans. Thyroid Cartilage.
44. 3. The inferior portion of the larynx is composed of the
A. thyroid cartilage
B. hyoid bone
C. glottis
D. cricoid cartilage
45. 4.Indication of Tracheostomy .
A.Acute Epiglotitis.
B.Maxilofacial Trauma.
C.Laryngeal Malignancy.
D.Extensive Lung Consolidation.
E.Coma.
46. 4.Indication of Tracheostomy .
A.Acute Epiglotitis.
B.Maxilofacial Trauma.
C.Laryngeal Malignancy.
D.Extensive Lung Consolidation.
E.Coma.
Ans.All
47. 5.Usual site of Tracheostomy?
48. Ans.2-3 or 3-4 Tracheal ring.
49. 6.Function of Tracheostomy Tube ?
A.Bypass Uper Airway Obstruction.
B.Increase Anatomical Dead Spase.
C.Increase Airway resistance.
D.Allow Frequent Airway Suction.
E.Protect Airway from Aspiration.
50. Ans.
A.Bypass Uper Airway Obstruction.
D.Allow Frequent Airway Suction.
E.Protect Airway Aspiration.
B.Decrease Anatomical Dead Spase.
C.Decrease Airway resistance
51. THANKS