Download
1 / 16
170 likes | 429 Vues
Localised Prostate Cancer: Is Active Surveillance the “Preferred” Option?. Simon F Brewster Oxford, UK. Active surveillance (AS) is the “preferred” option for men with *low-risk localised prostate cancer who are candidates for radical treatment (UK NICE Guidelines, 2008)

E N D
Localised Prostate Cancer:Is Active Surveillance the “Preferred” Option? Simon F Brewster Oxford, UK
Active surveillance (AS) is the “preferred” option for men with *low-risk localised prostate cancer who are candidates for radical treatment (UK NICE Guidelines, 2008) *PSA <10ng/ml + Gleason score ≤6 + T1-2a • There is a rising trend of observation in UK (BAUS database)
Observation of localised prostate cancer +/- delayed palliative treatment (watchful waiting) : the evidence • Competing risk analysis (Albertsen, 1998) • Estimated risk analysis for screen-detected disease (Parker, 2006)
Localised prostate cancer: Advantages of AS • Addresses overdetection of indolent disease : • Gap between diagnosis/incidence (12%) & mortality(3.5%) • 20% in clinical setting; 49% in screened patients (Kattan, 2003; Steyerberg 2007) • Reduces overtreatment of indolent disease : • Swedish randomised study (Bill-Axelson, 2005): NNT by RP = 17 to prevent one cancer death • AS avoids or delays treatment morbidity • Maintains QOL • Reduces healthcare spending?
Limitations of current AS evidence-base • 5 small non-randomised trials • Short follow-up • Lack of standardised inclusion criteria • Lack of standardised follow-up protocol • No consensus on triggers for intervention
Concerns with AS 1: Does delayed treatment reduce the chance of cure? • Delayed prostate cancer surgery for men with small low-grade prostate cancers does not appear to compromise curability (Johns Hopkins criteria) (Warlick, 2006) • Toronto AS series: 2/299 patients died of prostate cancer; 24 patients underwent radical prostatectomy: 14 (58%) had pT3a-c; 2(8%) had N1 disease. “For a group of patients with favourable clinical characteristics, this is a high rate of locally-advanced disease”. (Klotz, 2006) Answer: Unclear
Concerns with AS 2: Can we predict progression in AS patients? • All under investigation/validation in prospective studies: • Clinical features: DRE • PSA kinetics: doubling time or velocity • PSA density • Biopsy features: number of cores; core length • Other biomarkers in biopsy material e.g. p53, DNA arrays • Nomograms to predict insignificant disease Answer: Not very well at present
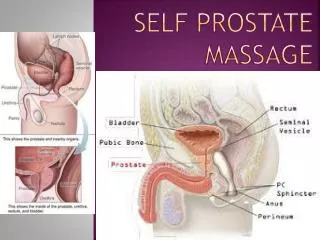
DRE surveillance • The only way to physically assess the prostate in clinic • Limitations include: • inter-observer variability • Difficulty in estimating nodule size • Difficulty in palpating the entire posterior surface
Prediction of insignificant disease by nomograms (Kattan, J Urol 2003, 170: 1792; Steyerberg, 2007) BUT ...Insignificant disease at biopsy is often significant after saturation biopsy or radical prostatectomy (Allan, 2003; Boccon-Gibod, 2005; Tsang, 2008; Abouassaly, 2008)
PSA kinetics: velocity and doubling time • PSA velocity: • PSAV >2 ng/ml in the year prior to radical treatment associated with ↑ risk of treatment failure and shorter survival. (D’Amico, 2005); • Often not known at diagnosis; • Is likely to be affected by the (BPH) volume of the gland; • PSA doubling time: • Toronto series: median doubling time = 7.0 years; • 42% >10 years; 20% >100 years; 20% <3 years (Klotz, 2006). • cut-offs for recommending active treatment vary: 3 or 4 years; • Swedish screen-detected disease: < 2 years associated with relapse following delayed treatment of; >4 years carried no risk of relapse (Khatami, 2006)
PSA density (PSA / TRUS-prostate volume) • Diagnostically, PSAD >0.15 associated with ↑ risk of cancer (Benson, 1982) • Subject to physiological fluctuations and inter-observer variations; • PSAD correlates with features of prostate cancer aggressiveness: • >0.19: ↑ risk non-confined (45%), Gleason 7+ (45%), cancer volume >5 c.c. (46%), progression after RP (21%). • <0.1: only 18% non-confined, Gleason 7+ only 20%, cancer volume >5 c.c. only 20%, progression after RP only 6%. • <0.15 predicts “insignificant” disease at radical prostatectomy (Allan, 2003); • During AS: PSAD at initial biopsy >0.9 predicts ↑ PSA velocity follow-up (Venkitaraman, 2007)
Concerns with AS 3: how do patients tolerate it? Psychological effects: satisfaction vs. anxiety • 2365 men, those receiving active treatment significantly more satisfied than those receiving no treatment (SEER, Hoffman, 2003) • Psychosocial barriers may be alleviated by good communication/ education/empowerment/peer-support groups (Pickles, 2007) • 329 men, anxiety/depression scores no different between patients on AS (n=100) compared to those receiving/received radiation therapy (Burnet, 2007) Answer: Uncertain
Concerns with AS 4: How safe is it? • AS appears safe for most patients based on the existing short-term non-randomised cohort studies • Web-based prospective validation of AS: the PRIAS study • Lack of randomised trials: 3 in progress • only Canadian START rigorously tests AS vs treatment in phase III randomised setting; • US PIVOT and UK Pro-tecT trials contain observation arms, but do not set out to treat all patients with curative intent. • UK NICE Guidance AS recommendation quickly criticised for lack of consensus and evaluation (Wilt, 2008). Answer: Uncertain
Conclusions • Yes, Active Surveillance is an option for low-risk localised prostate cancer, to reduce over-treatment, it’s morbidity and cost; • Patients should be informed of the uncertainties; • AS will become more prevalent in the future if/when population-based screening programmes are developed; • Careful patient selection and follow-up is important to minimise risk of on-surveillance disease progression; • Identification of early predictors of significant disease or progression will facilitate decision-making and minimise risk of harm; • Randomised trials are awaited to prove AS is as oncologically safe as active treatment.



![EVM System Surveillance Presented By: [NAMES] Presented to: [GROUP]](https://cdn0.slideserve.com/294105/slide1-dt.jpg)