Acut e Appendicitis
Acut e Appendicitis. Epidemiology. It affects 6~7 % of the population. Peak incidence in adolescents and young adults, with a slight male predominance in this age group. Infants, elderly, pregnant women and immunocompromised patients tend to


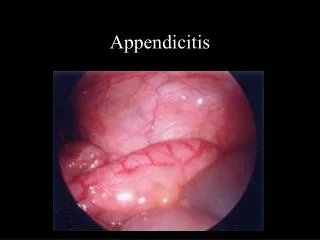
Acut e Appendicitis
E N D
Presentation Transcript
Epidemiology • It affects 6~7 % of the population. • Peak incidence in adolescents and young adults, with a slight male predominance in this age group. • Infants, elderly, pregnant women and immunocompromised patients tend to have atypical presentations and have higher morbidity and mortality.
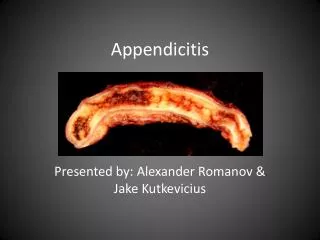
Pathophysiology • Obstruction-most commonly secondary to fecalith in adults and lymphoid hyperplasia in children. • Continued mucosal secretion. • Worsened edema, high luminal pressure and bacterial proliferation. • Transmural necrosis and bacterial penetration.
Clinical presentation • Classical presentation occurs in only 50 % of patients. • Pain begins in peri-umbilical or epigastric region, due to appendiceal distension and referred pain. • Pain localizes to the RLO as the parietal peritoneum in the area becomes irritated. • Anorexia and nausea occur almost uniformly after the pain.
Physical examination • Mild fever may be present. • Mc-Burney’s point • Rovsing’s sign • Psoas sign & Obturator sign • Rectal examination
Laboratory and Imaging Findings • WBC elevation from 10000 to 18000/mm3 • Abdominal radiograph may show a fecalith in the RLQ, loss of the psoas shadow and/or a few dilated loops of the bowel. • Ultrasonography reveals a non-compressible, aperistalic appedix larger than 6 mm in diameter.
Treatment • Immediate operative treatment is indicated. • In the case of a perforated appedix with phlegmon formation, an “interval” appedectomy is usually performed with drains left and skin & subcutaneous tissue open for weeks. • Peri-operative antibiotics have been shown to lower the infectious complications.
Prognosis • The mortality of appedicitis is the mortality of delay. • Most surgeons are therefore believed that a certain number of negative explorations are necessary to avoid a high incidence of perforation and its sequelae. • Can negative laparotomy be lowered without a concomitant rise in perforation rates?
The value of 99mTc HMPAO labeled white blood cell scintigraphy in acute appendicitis patients with an equivocal clinical presentation Eur J Nucl Med (2001) 28:575-580
Introduction • Up to 30% of patients with proved appendicitis are misdiagnosed and discharged. • The rate of normal appendectomy averages 16%, with females comprising 68% of these patients.
Materials and methods • This study was designed as a prospective clinical trial. Forty-one patients (24 females and 17 males, aged 7-70 years) were included. The inclusion criteria were acute right lower quadrant abdominal pain with a clinical presentation equivocal for acute appendicitis, as determined by the surgeons. • A WBC count of greater than 3000/mm3 was required for cell labeling.
Labeling of WBCs • Imaging The anterior abdomen and pelvis were imaged under a camera (Toshiba GCA 602) equipped with a low-energy all-purpose collimator starting at 30 min following the injection of 125-300 MBq 99mTc-HMPAO WBCs. Imaging was repeated at 1, 2, and 4 h.
Interpretation Negative: Absence of abnormal intra-abdominal localization through 4 h of imaging. Positive: Focal accumulation of 99mTc-HMPAO WBCs in the right lower quadrant. • Decision on surgical intervention was made on the basis of consensus between the two surgeons. • Non-operated patients was followed for a minimum of 1 month.
Discussion • There were no false-positive or false- negativeresults in this study.* • We believe that as the number of the patients studied increases, we may encounter false- positive results due to other diseases which cause right lower quadrant inflammation. • False-negative results can result when the activity of the appendix superimposed with the background, such as iliac vascular activity. This can be prevented by an oblique imaging technique.
In our group of patients with presentations equivocal for acute appendicitis, the negative laparotomy rate was only 5.8%. • Fasting reduce the enterohepatic circulation of the by-products of HMPAO metabolism and that this increased the specificity of the test.
Conclusion • 99mTc-HMPAO is a rapid and accurate method for detecting acute appendicitis in patients with an equivocal clinical presentation, which may reduce the hospital stay and lower unnecessary laparotomy rate.