Download

1 / 51
510 likes | 874 Vues
Burns. Can be caused by thermal, electrical, chemical, or UV radiation exposure More than 80% of burns occur in the home Extent of injury is function of temperature and duration of exposure.Cell damage occurs as a result of protein denaturation. Classification of Burns. Classified primarily accor

E N D
1. MINOR BURNS AND SUNBURN
2. Burns Can be caused by thermal, electrical, chemical, or UV radiation exposure
More than 80% of burns occur in the home
Extent of injury is function of temperature and duration of exposure.
Cell damage occurs as a result of protein denaturation
3. Classification of Burns Classified primarily according to depth
Classification as first, second, or third degree is obsolete
Replaced by superficial, superficial partial-thickness, deep partial-thickness, and full-thickness
The American Burn Association classifies burns as minor, moderate, or severe using depth, location, cause of burn, and body surface area (BSA) as criteria.
4. Assessing the area and degree of burns :
Burns are usually describe and evaluated on the basis of the area of the body affected and depth of penetration of the burn in the skin. This helps determine the necessary treatment regimen and weather self treatment, physician outpatient treatment or hospitalization is required.
The "rule of nine" is a rapid method of estimating the percentage of the body Surface involved in a burn wound.
.The body surface is divided in to 11 areas; each representing about 9 % of the total
5. Rule of nines Body Area
Arm 9%
Head 9%
Leg 18%
Anterior Trunk 18%
Posterior Trunk 18%
Perineum 1%
6. Superficial Burns Involves only the epidermis
Redness, warmth, and slight edema
Usually no blistering
May be painful because sensory nerve endings are intact
Most sunburns are classified as superficial
Most can be treated in outpatient setting or through self care.
Will heal within 3 to 6 days
7. Superficial Partial-Thickness Burns Damage to the outer epidermal layer
Often moist and weeping, painful blistering
Will blanch with pressure
Painful and sensitive to temperature and air
Healing occurs within 2 to 3 weeks
Small burns (1-2% BSA) of this type can be treated through self care
8. Deep Partial Thickness Burns Damage to the dermis layer
May appear as patchy white to red area
Large blisters may be present
May take up to 6 weeks to heal
Patients should be examined in a hospital emergency room immediately Blanching indicates loss of blood vessels to the area.
Pain may be more intense because of irritation to nerve endings
May cause thick scar formation, as well as contractures to the skin
Can convert to full thickness burns if not properly and promptly managed.Blanching indicates loss of blood vessels to the area.
Pain may be more intense because of irritation to nerve endings
May cause thick scar formation, as well as contractures to the skin
Can convert to full thickness burns if not properly and promptly managed.
9. Full Thickness Burns Dermis and epidermis destroyed
Skin appears dry, leathery that is painless, insensate
Wound may initially appear red but will fade to white over 24 hours
Healing occurs over months and hospitalization is normally required.
10. Infection of burns:
Burned skin is a good culture medium for microorganisms since:
there is much necrotic tissue ,
defense mechanisms are impaired by he occluded vascular circulation
-infection by gram +ve bacteria (staphylococcus, streptococcus) occurs during the first day. After the third day, gram �ve bacteria (mainly pseudomonas) predominate and can convert a second degree burn to third degree. Topical therapy with silver sulfadiazines, silver nitrate or antibiotics is essential.
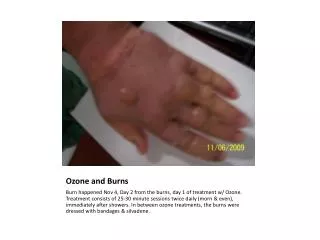
11. Treatment of burns
Minor burns:
They include first or second degree burn of less than 15 % of the body surface.
These can be treated on outpatient basis.
Application of local anesthetics to alleviate pain and antimicrobial agents to prevent secondary infection, are the basic element to treatment such burns. They should in suitable dosage forms.
Ointments, because of their greasy base facilitate microbial contamination, and require removal before further local treatment can be given.
Creams, solutions and sprays are easier to remove and, by cooling relief pain.
12. Severe burns: 50 % third degree. Thus require hospitalization where massive I.V. fluid are given, invasion controlled, recovery problem treated, skin skin grafting and rehabilitation of he patient is performed.
Over treatment of burns by applying substances or chemical other than the readily available, and valuable cold water is dangerous because of difficulty of removing contaminatioues for further treatment (e.g. skin grafling by surgeons). Toxic chemical may be absorbed or may cause allergic hypersensitivity reactions. The residue of chemicals may favor the growth of microorganisms.
13. Ingredients of OTC:
Local anesthetics e.g. benzocaine (0.5-20%) in burns with disrupted skin, lower concentration could be used (no penetration resistance)
Antimicrobials:
Compounds:
-QUAT (quaternary ammonium)
- benzalkonium chloride
-phenols and topical antibiotics
-mix of neomycin, polymyxin B sulfate and bacitracin
14. Photosensitive Reactions
Phototoxicity
Appears as exaggerated sunburn
Mostly caused by systemic medications including tetracycline, furosemide, phenothiazines, fluoroquinolones,
5-FU, and amiodarone Photoallergy
Relatively uncommon and appears as intensely pruritic eczematous dermatitis
Caused by sulfonamides, phenothiazines, thiazide diuretics, piroxicam, and cosmetics that contain certain fragrances.
24. Sunburn (dermatitis actinica)
It is acute inflammatory skin reaction resulting from sunburn or drug photosensitization caused by chemicals unusual sensitivity (persons suffering hypersensitivity)
Ultraviolet light is responsible for sunburns and suntan and increases in the risk of the basal cell carcinoma and malignant melanoma.
25. ULTRAVIOLET RADIATION SPECTRUM UVA (Longwave Radiation)
Range 320-400 nm
Erythrogenic activity is weak, however penetrates dermis
Responsible for development of slow tan tttl tan
Most drug-induced photosensitivity occurs in
26.
Uv is divided into three ranges:
UVA 320-400 nm (augment the effects of UVB)
UVB 290-320 nm
UVC 100-290 nm
UVB is the primary cause of sun burning. Premature aging and development of skin cancer.
-One of the body defence is the production of melanin (a pigment that result in darkening of the skin. individuals variability in melanin production and taning depends on: skin color and genetic factors.
27. Long-term hazards of skin damage from radiation:
Malignancy:
Squamous cell epithelioma
Actinic keratosis
Basal cell carcinoma
Premature aging
nevus, seborrheic keratosis, solar lentigo
wrinkles, lines, etc
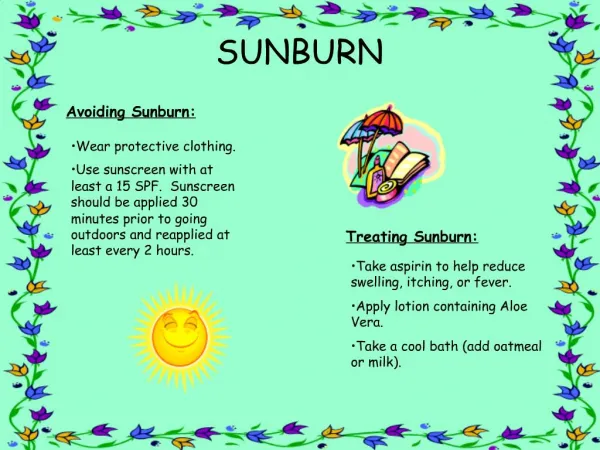
28. Sunscreen is cosmetic formulations that block UV rays.
Sunscreen is assigned sun protection factors or SPF, ratings that are supposed to indicate the level of the protection from UV radiation.
Sunburns: is an inflammatory alteration of normal skin that occurs following an excessive exposure to natural or artificial sunlight
Sunburns are redness, pain, as skin heals ---- skin will peel within one weak and itching.
29. Prolonged exposure second degree burn. Blistering of the skin, severe pain accompanied by prostaglandin release nausea and vomiting, so non steroidal anti-inflammatory will ameliorate the condition.
Multiple exposure premature aging and may lead to skin cancer.
30. Suntanning darkening of the skin in response to exposure to UVB. The darkening is caused by, an increased release of the pigment melanin in to the cells of the skin which is produced by the melanocytes cells (which is present in the basal layer of the skin epidermis and protects the body by absorbing harmful solar radiation .
Photosensitivity:
Is an abnormal reaction in the skin exposed to sun. It may be caused by numbers of substances that come in contact with the skin or are taken orally examples:
31. Oral photosensitivity topical photosensitivity
chlorothiazide antifungal
furosemide coal tar
Hydrochlorothiazide sunsueed agent e.g.
-antifungals paraamino benzoic A
Guiseofulvin
-antimicrobial
Quinolones
Sulfonamide
Tetracycline
32. Photosensitivity is classified into phototoxic reaction and photo allergic.
The two reactions involve the presence of: photo sensitizer plus sun and UVR
. Phototoxic -Non immunogenic 2 to 6 hour after exposure -Immediate reaction depends on the concentration of the photo sensitizer -causing a sun burn type Y reaction
33. Photoallergic - occurs only in the people previously sensitizer by a photoallergen -Typically occurs after 24-48 hours (delayed reaction) after sun exposure.- Not concentration dependent. The two reactions are confined to the sun exposed areas, face, neck hands and legs
34. Sunscreen preparation:
They are topical preparations that block the effect of the UVR on the skin by: either absorbing, reflecting or scattering UVR.
They are divided into physical and chemical sunscreens (on the basis of their mechanisms of actions)
35. Chemical sunscreens -they are aromatic compounds conjugated with a carbonyl group -these chemical absorb high intensity UV with excitation to a higher energy level.-this energy will be dissipated and converted to the ground state in the forms of (florescence , phosphorescence and chemical reaction)-so, they contain agents that absorb UV spectrum of coverage Disadvantages:-some are a photosensitize e.g. amino benzoic acid and benzophenons
36. Physical sun screens -they affect or scatter UV radiation -they are opaque -reflect , absorbed or scatter-they have broad spectrum -acts a physical barrier Disadvantages:Cosmetically unacceptable as they are visible, difficult to remove and discolor clothes e.g. titanium dioxide and zinc oxide (reflects and scatters UV visible light)
37. Sun Protection Factor (SPF) =
MED of Photoprotected Skin
MED of Unprotected Skin
MED is minimum dose of radiation which produces erythema
SPFs are determined indoors using xenon lamps which approximate the spectral quality of UV radiation
38. effectiveness of SPFs
Factors which influence Difference in skin types.
Thickness of the applied sunscreen.
Time of day.
Altitude: each 1,000 ft increase adds 4% to the intensity of erythema producing UV radiation; thus intensity is about 20% greater in Pocatello than at sea level.
Environment: snow/white surfaces reflect 70-90%, and when directly overhead water reflects nearly 100% of UVR.
Vehicle: determines skin penetration of sunscreen.
39. Uses:
- Sunscreen agents prevent and protect cell carcinoma in animals
-regular uses in human protect the skin forms:
Actinic keratosis , solar elastosis ,squamous cell carcinoma and -also prevent people sufferings from drug phosphosensitivity
ome will retain effect for 80 minutes i.g. very water resistance
40. -Evaluation of sunscreens: FDA evaluate them for their SPF and substantively
Substantively:
Refers to the ability of the product to adhere to the skin in the presence of sweating and swimming.
Water resistance products is essential for returning their photo protective effect up to 40 minutes of active immersion in water (
41. How we will increase substantively 1- It is either function of the formulations itself (sunscreen agail)
Recently, they introduce into the molecules of the agent, a sulfonium or quarternary ammonium function group to bind with the negative group sites of the epidermis.
Reservoir type sunscreen (penetrates and acts as a reservoir)
42. 2- SPF: the sun protective factor has been developed as a means of numerically identifying the efficiency of various sunscreen products and to provide for consumers a guide to the suitable products for particular types of the skin.
The SPF has been defined as:
The ratio between MED in protective skin (protect by the sunscreen protect) to the MED in the unprotected skin
MED in the protected skin
SPF = -------------------------------------
MED in unprotected skin
The larger SPF, the greater the protection the sunscreen can confer.
It reflects how long one can safely remains in the sun.
43. N.B higher SPF than 30 will not recommended as they require an increased amount of active ingredients which may irritate the skin and not provide much mare protection
44. -Evaluation of sunscreens: FDA evaluate them for their SPF and substantively
Substantively:
Refers to the ability of the product to adhere to the skin in the presence of sweating and swimming.
Water resistance products is essential for retuning their photo protective effect up to 40 minutes of active immersion in water (
46. Sun screen agents PABA (Para-aminobenzoic acid)
Very effective in the UVB range (200-320 nm).
Most effective in conc of 5% in 70% ethanol.
Maximum benefit when applied 60 min prior to exposure (to ensure penetration and binding to stratum corneum).
Does NOT prevent drug/chemical-induced photosensitivity rxn.
Contact dermatitis can develop.
May produce transient drying/stinging from alcohol content (may be alleviated by adding 10-20% glycerol).
47. PABA Esters (Padimate A, Padimate O, Glyceryl PABA)
Also very effective in UVB range (280-320)
Most effective in conc. 2.5-8% in 65% alcohol
May penetrate less effectively than PABA
Similar application and adverse effect
Less staining
48. Benzophenones (oxybenzone, dioxybenzone, sulisobensone)
Slightly less effective than PABA.
Absorbs from 250-400 nm spectrum (ie, UVA & UVB).
Combined with PABA or PABA ester improves penetrationand is superior to either agent used alone (200-400 nm wavelength coverage).
Beneficial in preventing photosensitivity rxns.
Contact dermatitis is rare.
49. Cineastes and Salicylates
Minimally effective, absorb UVB spectrum.
Generally used in combination with one of the above.
50. HIGH SPF SUNSCREENS Can achieve higher SPF by combining two or more agents.
SPF 30 (3%) vs 15 (6%) of radiation penetrating skin.
51. Physical sunscreen agent: protect against UVA + UVB therefore they classified as broad spectrum agent e.g. :
Titanium dioxide and zinc oxide
Titanium dioxide is ideal, chemically inert safe, reflect full UV spectrum
-by micronizing the element, it will be less viscible on the skin surface (broad spectrum agent)
-they are opaque and therefore less cosmetically acceptable than chemical sunscreens
-usually, they are applied over limited areas (e.g. the nose and lips)