Download

1 / 29
310 likes | 723 Vues
Venous thromboembolic diseases: Deep vein thrombosis. Support for education and learning slide set. 2013 NICE clinical guideline 144. What this presentation covers. Background Scope Recommendations Discussion NICE quality standard NICE Evidence Services NICE Pathway Find out more.

E N D
Venous thromboembolic diseases: Deep vein thrombosis Support for education and learning slide set 2013 NICE clinical guideline 144
What this presentation covers • Background • Scope • Recommendations • Discussion • NICE quality standard • NICE Evidence Services • NICE Pathway • Find out more
Glossary • INR: International normalised ratio • VTE: Venous thromboembolism • PE: Pulmonary embolism • DVT: Deep vein thrombosis • CTPA: CT pulmonary angiogram • V/Q SPECT: Ventilation perfusion scan • PTS: Post-thrombotic syndrome • VKA: Vitamin K antagonist • UFH: Unfractionated heparin • LMWH: Low molecular weight heparin
Definitions • Provoked DVT or PE: DVT or PE in patients with recent occurrence of major clinical risk factor for VTE • Proximal DVT: DVT in popliteal vein or above • Renal impairment: eGFR of less than 90 ml/minute/1.73 m2 (see notes) • Unprovoked DVT or PE: DVT or PE in patients with no recently occurring major clinical risk factors for VTE or patients with active cancer, thrombophilia or family history of DVT (these are risks, but they are constant) • Wells score: clinical prediction rules for estimating probability of DVT and PE
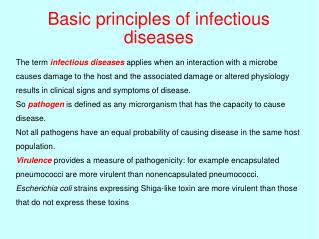
Background • Thrombus (blood clot) forms in a vein • Deep vein thrombosis – in deep veins of leg or pelvis • Pulmonary embolism – thrombus dislodges and travels to pulmonary arteries • Term ‘venous thromboembolism’ includes DVT and PE • Risk factors include: thrombophilia, history of DVT, surgery, obesity, acute illness, cancer and immobility • 500,000 people in Europe die from preventable hospital-acquired VTE every year
Scope • Guidance on management of VTE, investigations for cancer in patients with VTE and thrombophilia testing • Covers adults with suspected or confirmed DVT or PE • Includes advice on the Wells score, D-dimer measurement, ultrasound and radiological imaging • Does not cover those younger than 18, or women who are pregnant
Recommendations for DVT • Diagnostic investigations and diagnosis • Treatments: • pharmacological interventions • thrombolytic therapy • mechanical interventions • Patient information • verbal and written • self-management • Investigations for cancer • Thrombophilia testing
Diagnostic investigations (1) If a patient presents with signs or symptoms of DVT, carry out the following to exclude other causes: • an assessment of their general medical history and • a physical examination. If DVT is suspected, use the two-level DVT Wells score.
Diagnostic investigations (2) Wells score = DVT unlikely Offer a D-dimer test and if the result is positive, offer either: • proximal leg vein ultrasound scan (within 4 hours of request) or • if proximal leg vein scan not available within 4 hours, interim 24-hour dose of a parenteral anticoagulant followed by proximal leg vein ultrasound within24 hours of request.
Diagnostic investigations (3) Wells score = DVT likely Offer either: • proximal leg vein ultrasound scan (within 4 hours of request), if negative, a D-dimer test or • if proximal leg vein scan not available within 4 hours, D-dimer test and an interim 24-hour dose of a parenteral followed by proximal leg vein ultrasound within 24 hours of request Repeat proximal leg vein ultrasound scan 6–8 days later for all patients with positive D-dimer test and negative proximal leg vein ultrasound scan.
Diagnosis Diagnose DVT and treat patients with positive proximal leg vein ultrasound Take into consideration alternative diagnoses in patients with: • unlikely two-level DVT Wells score and negative D-dimer test or positive D-dimer test and negative proximal leg vein ultrasound scan • likely two-level DVT Wells score and negative proximal leg vein ultrasound scan and negative D-dimer test or repeat negative proximal leg vein ultrasound scan.
Pharmacological interventions (1) Confirmed PE or proximal DVT Offer low molecular weight heparin (LMWH) or fondaparinux as soon as possible, unless: • severe renal impairment • increased risk of bleeding • haemodynamically unstable Confirmed PE or proximal DVT and active cancer Offer LMWH, continue for 6 months
Pharmacological treatment (2) Confirmed PE or proximal DVT Offer a VKA to patients with confirmed proximal DVT or PE within 24 hours of diagnosis and continue the VKA for at least 3 months
Thrombolytic therapy Consider catheter-directed thrombolytic therapy for patients with symptomatic iliofemoral DVT who have: • symptoms of less than 14 days’ duration and • good functional status and • a life expectancy of 1 year or more and • a low risk of bleeding.
Mechanical interventions (1) Temporary inferior vena caval filters: • offer to patients with proximal DVT or PE who cannot have anticoagulation treatment • consider for patients with recurrent proximal DVT or PE despite adequate anticoagulation treatment (after considering alternatives). Ensure strategy for removing filter at earliest possible opportunity is planned and documented when filter is placed
Mechanical interventions (2) Offer below-knee graduated compression stockings (ankle pressure greater than 23 mmHg) to patients with proximal DVT a week after diagnosis or when swelling is reduced sufficiently, and: • advise patients to continue wearing the stockings for at least 2 years • ensure that the stockings are replaced 2 or 3 times per year or according to the manufacturer’s instructions • advise patients that the stockings need to be worn only on the affected leg or legs.
Patient information: verbal and written • How to use anticoagulants • Duration of treatment • Possible side effects and what to do • Effects of other drugs, foods and alcohol • Monitoring • How anticoagulants may affect dental treatment • Taking anticoagulants if they are planning pregnancy or become pregnant • How activities may be affected • When and how to seek medical help
Patient information: self management Information and advice Patients on anticoagulant treatment should receive an ‘anticoagulant information booklet’ and an ‘anticoagulant alert card’ Advise patients about the correct application and use of below-knee graduated compression stockings Self-monitoring of INR Do not routinely offer to PE or DVT patients
Investigations for cancer (1) Offer all patients with unprovoked DVT or PE, who are not known to have cancer: • physical examination (guided by patient’s full history) and • chest X-ray and • blood tests (full blood count, serum calcium and liver function tests) and • Urinalysis.
Investigations for cancer (2) • First unprovoked DVT or PE? • No signs or symptoms of cancer based on initial investigation? • Over 40? Consider further investigations for cancer: • abdomino-pelvic CT scan • mammogram for women
Thrombophilia testing X Do not offer to patients who are continuing anticoagulation treatment X Do not offer to patients who have had provoked DVT or PE X Do not routinely offer to first-degree relatives of people with a history of DVT or PE and thrombophilia Consider for patients with unprovoked PE or PE if it is planned to stop anticoagulation treatment
Discussion • How can we modify our service to allow us to offer proximal leg vein ultrasound within 4 hours of request? • Do we have the appropriate systems in place to ensure patients with a proximal DVT receive the appropriate follow up to assess continuation of LMWH, VKA and replacement of below-knee graduated compressions stockings? • What referral systems do we have in place to facilitate the onward investigation for cancer and thrombophilia for patients with unprovoked DVT? How do they need to be modified to meet the NICE recommendations?
NICE quality standard for diagnosis and management of venous thromboembolic diseases • Published March 2013 • Defines clinical best practice within this topic area. • Provides specific, concise quality statements, measures and audience descriptors to provide the public, health and social care professionals, commissioners and service providers with definitions of high-quality care. • Covers the diagnosis and treatment of venous thromboembolic diseases in adults, excluding pregnant women. Click here to go to the NICE quality standard for management of venous thromboembolic diseases
NICE Evidence Services Visit NICE Evidence Services for the best available evidence on all aspects of VTE diseases Click here to go to the NICE Evidence Services website
NICE Pathway The NICE VTE Pathway shows all the recommendations in the VTE diseases and VTE: reducing the risk guidelines Click here to go to NICE Pathways website
Find out more Visit http://guidance.nice.org.uk/CG144 for: • the guideline • information for the public • costing report • audit support • baseline assessment tool • PE educational resource (training plan, slide set and clinical case scenarios) • DVT educational resource (training plan, slide set and clinical case scenarios) • podcast • two-level wells score templates
What do you think? Did the implementation tool you accessed today meet your requirements, and will it help you to put the NICE guidance into practice? We value your opinion and are looking for ways to improve our tools. Please complete this short evaluation form. If you are experiencing problems accessing or using this tool, please email implementation@nice.org.uk. To open the links in this slide, set right click over the link and choose ‘open link’
Additional slides • This additional slide contains the two-level DVT Wells score. • If you used the hyperlinks to the Wells score in the presentation, you have already visited this slide.
Two-level DVT Wells score Return to slide 8 ‘Diagnostic investigations (1)’