Download
1 / 112
1.17k likes | 1.52k Vues
Pharmacist Interactive Clinical Case Series (PICCS): Angina Pectoris. C. Michael White, Pharm.D., FCP, FCCP Professor, University of Connecticut School of Pharmacy . Outline and Approach to Case. Must be opened in “slideshow” for hyperlinks to work Read the case and the scenarios in the case

E N D
Pharmacist Interactive Clinical Case Series (PICCS): Angina Pectoris C. Michael White, Pharm.D., FCP, FCCP Professor, University of Connecticut School of Pharmacy
Outline and Approach to Case • Must be opened in “slideshow” for hyperlinks to work • Read the case and the scenarios in the case • Answer questions and make drug recommendations • Click on forward hyperlinks (Red Boxes) to follow through case based on your responses • Click on home hyperlink (Blue House Icon) to go back to the last correct step in the series
Just Another Day, When… • Bella Bush is a 76 year old female who comes into a hospital outpatient pharmacy on March 1, 2006 complaining of new onset shortness of breath which began as she was walking from her home about a mile away to the convenient store across the street from your pharmacy. She was going to get some cigarettes. The pharmacist comes to your cardiovascular care ambulatory clinic which is along side the pharmacy and asks for help. You help her right over to your clinic examination room and say: “Please lay down and lets talk for a minute. Have you ever had symptoms like this before?” and she says “Yes, two days ago I was working in the attic moving boxes and had the same type of thing happened.” At that time she laid down in bed and the shortness of breath resolved after about 10 minutes. You ask her if she can remember any other episodes and she says: “Now that you mention it, this has happened 4 or 5 times over the past couple months”. In all cases, the episodes went away within a few minutes of resting. You ask if she has any other symptoms aside from the shortness of breath and she says: “Yes, I have this squeezing feeling between my breasts, you know on the inside.” She says the chest pressure is a 4 out of 10. You ask if she has any symptoms when she isn’t exercising and she says no. [SELECT RED BOX]
Just Another Day (Continued) • You take a 12-lead ECG and it shows ST segment depression in leads I, AVL, v4, v5 and v6. You ask Ms Bush to just sit quietly for a few minutes. In 5 minutes you ask how she is doing and she says that her shortness of breath and chest tightness has resolved. She then says “Thanks for your help, well then, time to get my smokes.” You ask her to wait and tell her that she needs to see her doctor. She says she doesn’t have a real doctor just a psychiatrist but then says, “why should I”?. What should you tell Ms Bush? “These symptoms might be a disease called heart failure which could be very bad if you don’t get it checked out and have it treated.” “These symptoms might be angina and you could be at risk of a heart attack if you don’t get it checked out have it and treated.” “You might be having a heart rhythm disturbance and could be at risk of dying unless you get it checked out and treated right away.” [Click Here For Tutorial on ECG Reading] [SELECT ONE RED BOX]
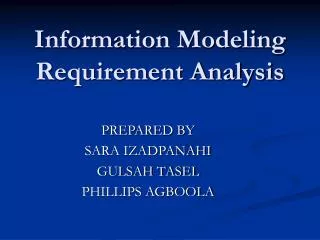
ECG: Ms Bush Reading: ST Depression Leads V4, V5 & V6 Shown by Arrows. While the ST Segment Depression is Up-Sloping in v4, it is Horizontal in the Other Leads Consistent With Ischemia. There are ST Depressions in I and AvL As Well But That is Not Shown Here V4 V1 V2 V5 V3 V6 [SELECT RED BOX]
ECG Reading Tutorial 1 • ST segment depressions or T-wave inversions suggest myocardial ischemia • ST depression is downsloping or horizontal in ischemia • Upsloping ST segment could be left ventricular hypertrophy, digoxin toxicity Downsloping Upsloping Horizontal [SELECT RED BOX]
ECG Reading Tutorial 2 • T-wave inversion • T-wave in opposite direction of QRS complex QRS Upright = R-Wave T-Wave in Opposite Direction = Ischemia T-Wave in Opposite Direction = Ischemia QRS Downward = S-Wave [SELECT RED BOX]
Isoelectric Line = J point Isoelectric Line = J point ST Segment Elevation (Convex Upwards) ST Segment Elevation (Concave Downwards) Isoelectric Line = J point ST Segment Elevation (Concave Upwards) ECG Reading Tutorial 3 • Convex Upwards or Concave Downwards ST segment elevation (>1mm) or new left bundle branch block suggests myocardial infarction • Need 3 criteria to diagnose MI: enzymes, injury current on ECG, and pain consistent with persistent chest pain Signs for Injury R and R’, Notched QRS Wider than Normal Not an ST Sign of Injury New Onset Left Bundle Branch Block [SELECT RED BOX]
ECG Reading Tutorial 4 • There are 12-leads on an ECG which can be used to determine location of left ventricular ischemia or injury current • They fall into four main zones Posterior v1-v4 Anterior v1-v4 Lateral I, AVL, v5, v6 [SELECT RED BOX] Inferior II, III, AVF
ECG Reading Tutorial 5 • Anterior zone of left ventricle (Front) • Looking at front surface of LV from leads v1-v4 (v1-v2, LV septum, v3, v4 pure anterior) • Ischemia show up as ST depression or T-wave inversion in v1-v4 • Infarction shows up as injury current (ST elevation) in v1-v4 [SELECT RED BOX]
ECG Reading Tutorial 6 Normally, in v1, v2, & v3, the QRS complex is first upward and then downward (R-S-wave), comes back to the isoelectric line and after a brief pause, the T-wave rises upright. Here the ST segment is convex upwards. This is anterior injury current. [SELECT RED BOX]
ECG Reading Tutorial 7 • Lateral Zone of LV (Left Side) • I, AVL, v5, v6 are the lateral leads • I, AVL is high lateral zone • v5 and v6 is low lateral zone • Inferior Zone of LV (Bottom) • II, III, AVF are the inferior leads • Posterior Zone of LV (Back Side) • v1 through v4 but shows reciprocal changes • Reciprocal change means ST elevation on back shows on anterior leads in front as ST depressions • So the ST depressions in v1-v4 could be a sign of anterior ischemia or posterior MI. Since posterior MI is rare, treat is if anterior ischemia until other 2 signs become apparent [SELECT RED BOX]
ECG Reading Tutorial 8:Inferior MI, See the Convex ST Elevations in II, III, AVF [Click on Blue Box to go Back]
Heart Failure • This is a good guess. Ms Bush has dyspnea on exertion which could be a symptom of left-sided heart failure. The chest tightness and the ST depression argues against it only being left-sided heart failure, however. Go back and try again. [Click on Blue Box to go Back]
Angina Pectoris • This is most likely correct. She has dyspnea on exertion and chest tightness which comes on during exercise and goes away with rest. About 25% of women over the age of 74 have dyspnea on exertion as their most pressing symptom when experiencing angina pectoris or a myocardial infarction but they frequently also have substernal chest pain. These events have been occurring for several months and show the same pattern of exertion onset and rest resolution which is consistent with angina pectoris. The ST segment depression also suggests myocardial ischemia. [SELECT RED BOX]
Arrhythmia • This is not correct. The symptoms Ms Bush has are more consistent with angina pectoris or left-sided heart failure than with an arrhythmia. Dizziness and palpitations would be the more likely symptoms of arrhythmias such as atrial fibrillation or flutter. [Click on Blue Box to go Back]
Myocardial Ischemia Zone • You contact your physician collaborator, Anthony Canoli, MD and he asks what happened. You tell him and then give him the most likely diagnosis based on the information you have available. What do you think it is? Anterior angina pectoris involving the left anterior descending coronary artery Lateral angina pectoris involving the circumflex artery Inferior angina pectoris involving the left main coronary artery [SELECT ONE RED BOX]
Anterior and LAD • This is incorrect. If it was anterior ischemia the ECG during the event would most likely have shown ST segment depression or T-wave inversion in leads (v1 + v2) and/or (v3 + v4). Sole anterior ischemia would suggest a blockage in the left anterior descending (LAD) coronary artery. [Click on Blue Box to go Back]
Lateral and Cx • This is correct. An ECG taken at the time of lateral ischemia usually shows ST segment depression or T-wave inversion in leads I, AVL, v5 and v6. If you remember that the “L” in “AVL” stands for “Lateral” it can help to guide you. Sole lateral ischemia usually involves a blockage in the left circumflex (LCx) coronary artery. Since the left main (LM) coronary artery brings blood to both the left anterior descending and the LCx coronary arteries, a blockage in the LM could show up as antero-lateral ischemia (ST depressions in I, AVL, v1-v6). [SELECT RED BOX]
Inferior and LM • This is not correct. A patient with inferior ischemia would most likely have a 12-lead ECG which show ST segment depression or T-wave inversion in leads II, III, and AVF. If you remember that the “F” in “AVF” stands for “Foot” it can help to guide you. The coronary artery segment with a blockage responsible for inferior ischemia would most likely be in the Right Coronary Artery (RCA) but not always. A blockage in the Left Main (LM) would be more likely to cause antero-lateral ischemia than inferior ischemia. [Click on Blue Box to go Back]
One Week Later • 03/08/2006: Ms Bush has an appointment with Dr Canoli and the following is the medical record of that visit. Fill out your own monitoring form so you can continue on through the rest of the case. [SELECT RED BOX]
Patient Medical Chart: 03/08/06: Bella Bush is a 75 year old female who had a two month history of intermittent chest pain and shortness of breath brought on by exertion and relieved by rest. The ECG for the 03/01/06 episode showed lateral ST segment depression. Referred for Cardiologist work-up. PMH: Depression x3 years Meds on Admit: Nefazodone 200mg twice daily, amitriptyline 75mg twice daily. HPI: Ms. Bush’s blood work sent 03/02/06 (see laboratory section). Ms Bush had an angiogram on 03/05/06 which showed 80% blockage of the LCx. Percutaneous coronary intervention (PCI) was performed with two stents placed in the LCx. SH: Smokes 3 packs per day, consumes 7-8 drinks daily. [Click Here For Tutorial on Angiography and PCI] [SELECT RED BOX]
Angiography • Angiography • Catheter threaded through femoral artery into coronary arteries • Dye injected in coronary arteries • Areas of narrowing or blockage noted • Catheter inserted into left ventricle • Dye injected • Left ventricular ejection fraction (LVEF) determined by fraction of dye expelled when heart contracts • LVEF <40% = left ventricular dysfunction [SELECT RED BOX]
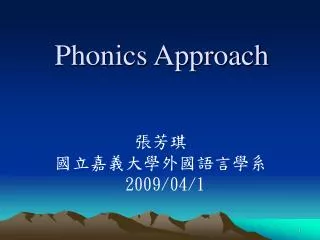
Angiography: Inject Dye in Coronary Arteries Angiogram showing blockage in the Right Coronary Artery. Blockage Denoted by White Arrow [SELECT RED BOX]
TIMI Blood Flow Staging TIMI 0 (No Flow) TIMI 1 (Trickle) TIMI 2 (Good Flow) TIMI 3 (Normal Flow) [SELECT RED BOX]
Stenting in PCI Stent InsertedStent Expanded on Balloon Stent Left In Vessel Actual Deployed Stent [SELECT RED BOX]
PCI Procedures Angiography Angioplasty + Stent Angiography TIMI 0 Flow PCI of Vessel TIMI 3 Flow Thrombolytic agents can reveal an underlying stenosis, which can then be treated with an adjuvant interventional treatment. [SELECT RED BOX]
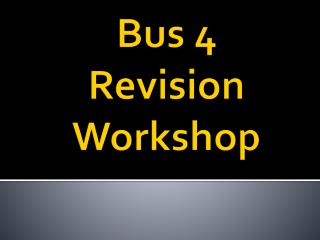
LV Gram: LVEF Determination Fluoroscopy: Targeted X-Ray Catheter Inserted in Left Ventricle (See how tip of pigtail catheter curls up showing you are in the left ventricle). Injecting Die Allows Determination of Left Ventricular Ejection Fraction [Click on Blue Box to go Back] Catheter Left Ventricle
Patient Medical Chart Continued FH: Husband died 3 years ago of lung cancer. Laboratory Data 03/03/06: Na 135mEq/L, K 3.8mEq/L, SCr 1.3mg/dL, glucose 142mg/dL, LDL cholesterol 176mg/dL, HDL cholesterol 62mg/dL, triglycerides 82mg/dL, AST 576mg/dL, ALT 615mg/dL. Physical Exam 03/02/06: HEENT normal, no abnormal heart sounds, no hepatomegaly, no jaundice, no spider angiomas, no JVD, no bruits, no ankle swelling. Weight 98 pounds, height 5 foot 6 inches. Blood pressure 178/85mmHg. Current Medications: Nefazodone 20mg twice daily, amitriptyline 75mg twice daily, aspirin 81mg. --- Anthony Canoli, MD [SELECT RED BOX]
Cardiology Clinic 03/9/06: Bella Bush is admitted to your clinic by Dr Canoli for chronic medical management of her angina pectoris. You ask her how she has been doing and she responds: “Oh, I still have some chest pain from time to time but I have to do more to bring it on than I used to”. What should you prescribe Ms Bush to treat acute anginal attacks? Nitroglycerin sublingual tablets 0.4mg PRN chest pain. Nitroglycerin lingual aerosol 0.4mg PRN chest pain Isosorbide dinitrate 20mg orally four times daily [SELECT ONE RED BOX]
Nitroglycerin Tablets • Good guess. While this choice is perfectly acceptable there is a chance that the anticholinergic effects of amitriptyline could make it harder to dissolve the tablets sublingually. As such, nitroglycerin aerosol might be better for this patient. [Click on Blue Box to go Back]
Nitroglycerin Aerosol • Good job! While it would not be wrong to select nitroglycerin sublingual tablets, the anticholinergic effects of amitriptyline might induce dry mouth and make it harder to dissolve the nitroglycerin tablets. [SELECT RED BOX]
Isosorbide Dinitrate • This is incorrect. Chronic isosorbide dinitrate would not be the best choice to treat acute attacks. You want a short acting agent on board such as sublingual nitroglycerin or nitroglycerin aerosol to use when acute chest pain events occur. [Click on Blue Box to go Back]
Clinic Visit 1 Continued • Ms Bush is given nitroglycerin aerosol 0.4mg PRN chest pain. What counseling should she be given? Remove the cap and spray the drug between your cheek and gum three times, if the pain persists after 5 minutes then drive to the ER, you are having a heart attack. Remove the cap and shake the can vigorously, breathe out all you can and then while inhaling slowly and consistently actuate the canister and breathe in the aerosol. When done, hold your breathe for a few seconds before exhaling. Wait 5 minutes and if your chest pain still persists, take another dose of nitroglycerin spray in the same manner. Wait another 5 minutes and if you still have chest pain, take another dose of the nitroglycerin spray and either call an ambulance or have someone take you to the ER because it might be something more serious than just angina and needs to be checked out right away. Remove the cap and do not shake the can. Open your mouth and apply one spray to your tongue. Repeat this at 5 minute intervals if the pain has not gone away for a total of three doses. If you still have pain you will need to go to the ER right away so call for an ambulance or have someone drive you in. You might be having a heart attack and if you are; the faster you come in, the more of your heart muscle can be saved from damage. [SELECT ONE RED BOX]
SL Nitro Aerosol • This is incorrect. The spray goes on your tongue not sublingually. You need to space out the sprays by 5 minutes to avoid hypotension. You don’t want to say that Ms Bush is definitely having a heart attack if the spray fails, there is only a chance that she is. Saying she definitely is having one could lead her to panic. [Click on Blue Box to go Back]
Inhaled Nitro Aerosol • This is incorrect. This is decent technique for a metered dose inhaler but not for nitroglycerin aerosol. You do not want to shake the canister before applying it and want to apply it to your tongue, not inhale it. [Click on Blue Box to go Back]
Lingual Nitro Spray • This is correct. You gave her good technique and made sure to let her know what to do if the three sprays were ineffective. This is the start of great pharmaceutical care. Some cardiologists recommend going to the ER if the second dose fails and taking the third dose on the way to save time. [SELECT RED BOX]
For the Stent • What other drug therapy does Ms. Bush need in order to reduce her chances of stent platelet-thrombus formation? Clopidogrel 75mg daily Amlodipine 10mg daily Warfarin 5mg daily to start and titrated to an INR of 2-3 [SELECT ONE RED BOX]
Clopidogrel • This is correct. The metal on the stents are a nidus for platelet aggregation until the endothelial lining overgrows the stent. ADP inhibitors such as clopidogrel and ticlopidine have been combined with aspirin in people with stents in order to reduce the chances of platelet-thrombus formation. Therapy with the combination should be continued for at least 3 months with a bare metal stent and continued out to a year based on the results of the PCI-CURE and CREDO studies. [SELECT RED BOX]
Amlodipine • This is incorrect. Amlodipine would not impact the risk of platelet-thrombus formation. [Click on Blue Box to go Back]
Warfarin • This is not a bad guess. Warfarin would have anticoagulant effects and could impact the formation of platelet-thrombus formation. The INR range is adequate. However, therapy with an ADP inhibitor such as clopidogrel and ticlopidine in addition to aspirin therapy would be superior drug therapy among patients who can take both drugs. [Click on Blue Box to go Back]
Visit 1 Part 3 • Ms Bush is given a prescription for clopidogrel 75mg daily. You then request that she receive laboratory testing of her TSH level. Why would you test her TSH? Hypothyroidism could cause depression Hyperthyroidism could worsen angina pectoris Hypothyroidism could worsen hyperlipidemia [SELECT ONE RED BOX]
Thyroid and Depression • While this is true, this is not the best choice. However, if hypothyroidism is found, then correction could lead to improvements in her mood and Ms Bush might not need two antidepressants in the future. [Click on Blue Box to go Back]
Thyroid and Angina • This is the best choice. While hypothyroidism can worsen depression and increase lipid concentrations, the main reason for checking Ms Bush thyroid function is to see if hyperthyroidism could be exacerbating her anginal episodes. However, if she has hypothyroidism, correcting it would be worthwhile for her other disorders as well. [SELECT RED BOX]
Thyroid and Hyperlipidemia • While hypothyroidism can exacerbate hyperlipidemia, this is not the best choice. However, correction of the hyperlipidemia could improve her lipid profile as well. [Click on Blue Box to go Back]
TSH Ordered • A laboratory slip is filled out so that Ms Bush can have her TSH checked. You ask Ms Bush about over the counter, herbal, and illicit product use. Why would you do this? You want to know if she is taking nonsteroidal anti-inflammatory drugs You want to know if she is taking stimulants like decongestants or Ma Huang (Ephedra) You want to know if she is taking St John’s Wort [SELECT ONE RED BOX]
What Non-Prescription Drugs are You Taking? • All of these choices are correct. Eliciting information on nonprescription drug intake is as important as asking about allergies. If she was taking nonsteroidal drugs it could be increasing her blood pressure. If she was taking stimulants it could increase her blood pressure and could cause vasoconstriction and exacerbate her angina. If she took St John’s Wort, she would have drug interactions with CYP and P-glycoprotein metabolized drugs. Ms Bush is taking a CYP 2D6 substrate (amitriptyline). [SELECT RED BOX]
OTC Use • The only nonprescription drug she takes is acetaminophen 500mg PRN pain. You ask her how she takes it and she says: “I take it for pain, I usually take 1 or 2 but a couple weeks ago I had a big headache before bed so I took 3 tablets. The pain didn’t go away in an hour so I took 3 more. The pain still didn’t go away after another hour so I took 4 more. That really fixed it.” [SELECT RED BOX]
Acetaminophen PRN • You let her know that you are concerned. You talk with her very seriously about about not taking that much acetaminophen. She is instructed to only take the recommended amount of drug. You let her know that the amount of acetaminophen she took could have hurt her liver, especially since she consumes so much alcohol. Ms Bush bursts into tears and tells you that things are hard since her husband died of lung cancer. She feels somewhat better while being treated with the antidepressants but alcohol takes the edge off. She says that she sees a psychiatrist but doesn’t tell him about the alcohol intake. You let her know that she needs to talk to her psychiatrist about it because she might not be getting the best drug therapy. She says she will. You amend her laboratory sheet so she will now receive a follow-up AST and ALT as well. You ask to see her back in your office in a month. [SELECT RED BOX]
First Follow-Up Visit • 04/12/06: Ms Bush comes in to see you. She has seen her psychiatrist and was switched from amitriptyline to fluoxetine 20mg daily. They set up a plan for her to gradually reduce her alcohol intake and she is now on alprazolam 0.25mg daily for her anxiousness. You ask about her angina and she responds: “I still get angina pain with exercise, it’s still better then before I got my stent and the nitro works pretty well.” [SELECT RED BOX]