Download
1 / 33
520 likes | 2.46k Vues
PULMONARY CIRCULATION, PULMONARY EDEMA, PLEURAL FLUID. Dr. Ayisha Qureshi Assistant Professor, MBBS, Mphil. OBJECTIVES. By the end of the lecture, you should be able to: Give the physiologic anatomy of the Pulmonary Circulatory System. Name the 2 types of blood supplies of the lung.

E N D
PULMONARY CIRCULATION, PULMONARY EDEMA, PLEURAL FLUID. Dr. Ayisha Qureshi Assistant Professor, MBBS, Mphil
OBJECTIVES By the end of the lecture, you should be able to: • Give the physiologic anatomy of the Pulmonary Circulatory System. • Name the 2 types of blood supplies of the lung. • Differentiate between the Pulmonary and systemic circulation. • Give the different pressures in the Pulmonary Circulation. • Name the different zones in the lungs on the basis of regional pulmonary blood flow and the effect of gravity. • Explain the pathogenesis of Pulmonary edema. • Give the significance of Pleural fluid and explain the pathogenesis of Pleural effusion.
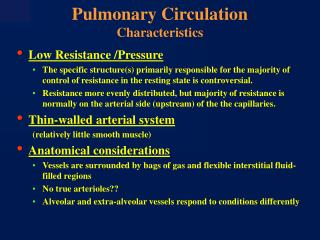
Comparison of the Pulmonary & Systemic Circulation PULMONARY CIRCULATION SYSTEMIC CIRCULATION HIGH PRESSURE - B/c it needs to send blood to the brain even when standing & to the tip of en elevated fingertip. HIGH RESISTANCE - because of increased smooth muscle in the arterioles & the metarterioles. LOW COMPLIANCE - because of resistance offered by the arterioles and the metarterioles. • LOW PRESSURE - because it only needs to pump blood to the top of the lungs. - if it is HI pressure, then following Starling forces, the fluid would flood the lungs. • LOW RESISTANCE - only 1/10th of the resistance of the systemic circ. - arterioles have less smooth muscle, veins are wider & shorter & pulmonary vessel walls are thinner. • HIGH COMPLIANCE - accommodates 5 L of blood (same as the systemic circulation) - Accommodates shifts of blood more quickly e.g. when a person shifts from a standing to a lying position
Advantages of Pulmonary Circulation being a Low Resistance system: • Accommodates more blood as a person shifts from the standing to the lying position. • High compliance allows the vessel to dilate in response to modest increase in Pulmonary arterial pressure. • Pulse pressure in the pulmonary circulation is rather low.
PRESSURES IN THE PULMONARY SYSTEM • Right Ventricle: Systolic= 25 mmHg Diastolic= 0-1 mmHg, • Pulmonary artery: Systolic= 25 mmHg Diastolic= 8 mmHg Mean Pulmonary arterial pressure= 15 mmHg. • Pulmonary Vein: Averages about 5 mmHg • Pulmonary capillaries: 7 mm Hg • Left atrium: Averages 2 mmHg
Important Points • The Pulmonary artery emerges from the Right Ventricle, follows the bronchial tree, bifurcates with it and enters the lung. When it reaches the alveoli, it forms a dense network of capillaries like a flowing sheet surrounding the alveoli so that efficient oxygenation of the blood can take place. • The veins that arise carry the oxygenated blood and form the Pulmonary Veins that take the blood to the Left Atrium. • The Bronchial artery emerges from the aorta and supplies the lung parenchyma and tissue. Deoxygenated blood is carried away by the veins. A small amount of bronchial blood drains into the azygous and hemiazygous veins. • At the level of the respiratory bronchioles, capillaries derived from the bronchial arteries anastomose with those derived from the pulmonary arteries. • Because veins of bronchial circulation drain into pulmonary veins, there is some venous admixture of the oxygenated blood in pulmonary veins and deoxygenated blood of the bronchial veins.
POINTS TO NOTE: • The average RBC spends 0.75 sec in the Pulmonary capillaries as it passes through at least 3 alveoli (can decrease to 0.3 sec during exercise). • 2 Lungs: 300 million alveoli 2 Lungs: 280 billion highly anastomosing capillaries • Effect of diminished alveolar oxygen on local alveolar blood flow: Unlike the rest of the circulatory system where the decrease in oxygen or metabolites leads to vasodilation of the vessels, in the pulmonary circulation, a decrease in oxygen uptake by the blood in the pulmonary vessels leads to pulmonary vessel vasoconstriction with an increase in the resistance. This effect of low oxygen on pulmonary vascular resistance has an important function: to distribute blood flow where it is most effective.
ZONES OF THE LUNGS The alveoli are NOT created equal when it comes to PERFUSION(Q) and VENTILATION(V). The Perfusion (Q) varies because of 2 reasons: • Posture • Gravity We can divide the upright Lung into 3 zones (some books say 4) based on the relationship between the following pressures: • Pa= Alveolar Air Pressure • PPA= Pressure in Pulmonary arterioles • PPV= Pressure in Pulmonary Veins Thus, standing on your head will reverse the flow-height relationship. POINT TO NOTE: Hydrostatic pressures in the Pulmonary vessels all continue to increase by 1 cm H20 for each 1 cm decrease in height from the level of the left atrium & continues to decrease by 1 cm for every 1 cm increase in height above the left atrium.
The Zones of the Lung and the Difference in Regional Blood Flow
Pathophysiology of the ZONES of the Lungs • Effect of Exercise: The blood flow in all parts of the lungs may increase during exercise. In the top of the lungs, the increase may be 700-800% while in the lower parts may be 200-300%. This is because during exercise pulmonary vascular pressures rise enough during the exercise to convert the lung apices from zone 2 to zone 3 pattern of flow. • Zone 1 Blood flow occurs only during Abnormal conditions. Usually this is not seen unless there are 2 condition: - if an upright person is breathing against a positive air pressure and the intra-alveolar air pressure is higher than normal. - in an upright person, pulmonary circulatory pressure is very low as seen after severe blood loss.
Total Outward Force + 29 mmHg Total Inward Force ‒ 28 mmHg MEAN ARTERIAL PRESSURE: +1 mmHg The normal outward forces are slightly greater than the inward forces, providing a mean filtration pressure at the pulmonary capillary membrane. This filtration pressure causes a slight continual flow of fluid from the pulmonary capillaries into the interstitial spaces, and except for a small amount that evaporates in the alveoli, this fluid is pumped back to the circulation through the pulmonary lymphatic system. This keeps the alveoli “DRY”.
PULMONARY EDEMA Definition: It is a condition in which fluid accumulates in the lungs. OR It is the effusion of fluid into the alveoli and the interstitial spaces of the lungs. Underlying Cause: Any factor that causes the Pulmonary Interstitial fluid pressure to rise from the negative range into the positive range will cause rapid filling of the pulmonary interstitial spaces & alveoli with large amounts of free fluid.
CAUSES OF PULMONARY EDEMA: • Left-sided heart failure or mitral valve disease (Most common). • Damage to the pulmonary capillary membrane caused by infections. e.g. pneumonia, inhalation of poisonous gases as chlorine or sulfur dioxide. This causes the leakage of the plasma proteins & fluids into the pulmonary interstitial spaces & alveoli that raises the Pulmonary Interstitial pressure. Safety Factor in Pulmonary edema: The plasma capillary pressure must rise from the normal value of 7 mmHg to above 28 mmHg (plasma colloid osmotic pressure) for edema to occur. So there is a safety factor of 21 mmHg.
Signs & Symptoms ofPulmonary edema: • Difficulty breathing • Coughing up blood (pink, frothy sputum) • Anxiety • Excessive sweating and pallor • Inability to lie down due to breathlessness • Signs of left ventricular failure like peripheral edema & raised JVP. • Respiratory failure • Death
Treatment: • Symptomatic treatment • High-flow oxygen therapy. • Diuretics to improve preload and afterload & aid in improving the cardiac function.
PLEURAL CAVITY The pleural cavity is the potential space between the two pleura (visceral and parietal) of the lungs. The pleura is a serous membrane which folds back onto itself to form a two-layered, membrane structure (like a balloon). It normally contains a thin layer of mucoid fluid. The outer pleura (parietal pleura) is attached to the chest wall. The inner pleura (visceral pleura) covers the lungs and adjoining structures, as blood vessels, veins, bronchi. The amount of fluid normally present is only a few millilitres. Thus, it is called a potential space as it is too narrow to be an obvious physical space.
Importance of Pleural Cavity • The normal collapse tendency of the lungs is ‒ 4 mmHg. Thus, the pleural fluid pressure must always be at least as negative as the pressure in the pleural cavity (‒ 4 mmHg) to keep the lungs expanded. • Actual measurement has shown it to be ‒ 7 mmHg. Thus, the negativity of the pleural fluid keeps the normal lungs pulled against the parietal pleura of the chest cavity.
PLEURAL EFFUSION Definition: Pleural effusion is accumulation of large amounts of free fluid in the pleural space. It is the same as edema fluid in the tissues & can be called “edema of the fluid”. Causes: Blockage of lymphatic drainage from the pleural cavity. Cardiac failure Greatly reduced plasma colloid osmotic pressure. Infection/ inflammation of the pleural surfaces causing leakage into the pleural cavity.
Signs & Symptoms of Pleural Effusion: • Shortness of breath (as the fluid in the pleural cavity increases, harder it becomes for the lungs to expand and more difficult for the patient to breathe). • Chest pain occurs as the pleural lining is irritated. It is a sharp pain that increases with a deep breath. • Sweating • Signs and symptoms of cardiac failure. • Weight loss. Treatment: • Symptomatic • ABC (airways, breathing, circulation) • Thoracocentesis • Chest tube to remove excess pleural fluid