Download
1 / 75
750 likes | 887 Vues
Discover how the kidneys regulate electrolytes, blood pressure, waste, and pH while maintaining fluid balance. Explore the anatomy, nephron function, and the intricate glomerular filtration process within our renal system.

E N D
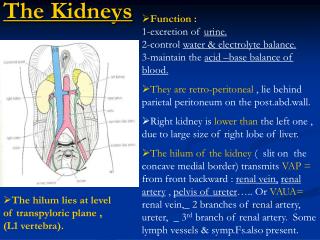
Kidney Function • Regulate ECF (plasma and interstitial fluid) through formation of urine and the concentration of ions in the ECF (Na+ ,K+ ,Cl- ,HCO3 ,Ca+2 ,Mg+2 ,SO4-2 ,PO4-3). • Primary function. • Regulate volume of blood plasma. • Blood Pressure. • Regulate waste products in the blood. • Regulate concentration of electrolytes. • Na+, K+, and HC03- and other ions. • Regulate pH (maintaining proper acid-base balance). • Secrete erythropoietin. • Maintain H2O balance in the body
Producing renin, an enzymatic hormone that triggers a chain reaction important in salt conservation by the kidneys. • Convert vitamin D into its active form
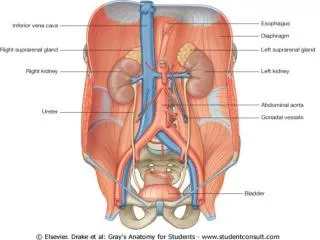
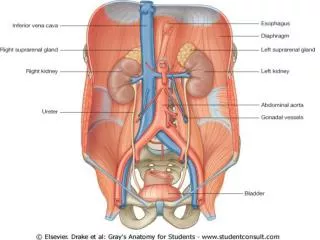
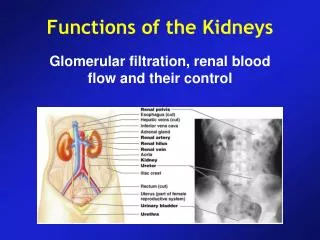
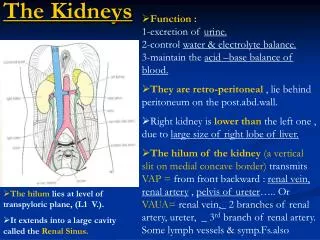
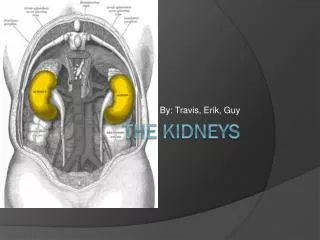
The urinary system consists of the urine-forming organs—the kidneys—and the structures that carry the urine from the kidneys to the outside for elimination from the body. The kidneys are a pair of bean-shaped organs about 4 in to 5 in. long that lie in the back of the abdominal cavity, one on each side of the vertebral column, slightly above the waistline.
Each kidney is supplied by a renal artery and a renal vein. After urine is formed, it drains into a central collecting cavity, the renal pelvis, located at the medial inner core of each kidney. From there urine is channeled into the ureter, a smooth muscle–walled duct that exits at the medial border in close
proximity to the renal artery and vein. There are two ureters, one carrying urine from each kidney to the single urinary bladder.
The urinary bladder, which temporarily stores urine, is a hollow, distensible, smooth muscle–walled sac. Periodically, urine is emptied from the bladder to the outside through another tube, the urethra, as a result of bladder contraction.
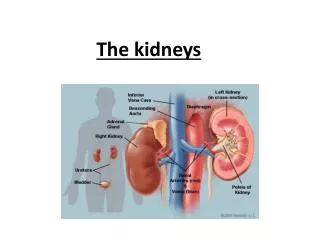
Structure of the Kidney • Outer cortex: • Contains many capillaries. • Medulla: • Renal pyramids separated by renal columns. • Pyramid contains minor calyces which unite to form a major calyx. • Major calyces form renal pelvis. • Renal pelvis collects urine. • Transports urine to ureters.
Micturition Reflex • Actions of the internal urethral sphincter and the external urethral sphincter are regulated by reflex control center located in the spinal cord. • Filling of the urinary bladder activates the stretch receptors, that send impulses to the micturition center. • Activates parasympathetic neurons, causing rhythmic contraction of the detrusor muscle and relaxation of the internal urethral sphincter. • Voluntary control over the external urethral sphincter. • When urination occurs, descending motor tracts to the micturition center inhibit somatic motor fibers of the external urethral sphincter.
Nephron • Functional unit of the kidney. • Consists of: • Blood vessels: • Afferent arteriole • Glomerulus • Efferent arteriole . • Peritubular capillaries. • Urinary tubules: • Boman’s capsule • Proximal convoluted tubule. • Loop of henle. • diatalconvoluted tubule. • Collecting duct.
The three basic renal processes are: • Glomerular filtration • Tubular reabsorption • Tubular secretion
Glomerular Filtration Membrane • Endothelial capillary pores are large fenestrae. • 100-400 times more permeable to plasma, H20, and dissolved solutes than capillaries of skeletal muscles. • Pores are small enough to prevent RBCs, platelets, and WBCs from passing through the pores.
Glomerular Filtration Membrane • Filtrate must pass through the: basement membrane: • Thin glycoprotein layer. • Negatively charged (The negatively-charged basement membrane repels negatively-charged ions from the blood, helping to prevent their passage into Bowman's space). Podocytes: • special cells which have numerous of pseudopodia (pedicles) that interdigitate to form filtration slits along the capillary wall.
Glomerular Filtration Membrane(continued) Insert fig. 17.8
Glomerular filter • The filtration surface is 1.5 square meter • Amount of the solution, which is filtered in glomerular apparatus is around 180-200 l. • The rest (97 %) has to be reabsorbed in the tubules back to the body, so the final volume of urine is around (1.5 - 2 l per day). • Depends on: • Pressure gradient across the filtration slit (pressure is the major force responsible for inducing glomerular filtration) • Blood circulation throughout the kidneys • Permeability of the filtration barrier • Filtration surface • The solution after filtration is very similar like plasma, but should be WITHOUT PROTEINS
Glomerular filter • Three physical forces are involve in glomerular filtration: • Glomerular pressure (increase filtration) • Plasma colloid pressure (opposes filtration) • Bowman’s capsule hydrostatic pressure (opposes filtration)
Glomerular Ultrafiltrate • Fluid that enters glomerular capsule is called ultrafiltrate. • Glomerular filtration rate (GFR): • Volume of filtrate produced by both kidneys each minute. • Averages 115 ml/min. in women; 125 ml/min. in men.
Regulation of GFR • Vasoconstriction or dilation of the afferent arterioles affects the rate of blood flow to the glomerulus. • Affects GFR. • Mechanisms to regulate GFR: • Sympathetic nervous system. • Autoregulation. • Changes in diameter result from extrinsic and intrinsic mechanisms.
Sympathetic Regulation of GFR • The sympathetic control of the GFR is aimed at the long-term regulation of arterial blood pressure. • Baroreceptors respond extremely rapidly to changes in arterial pressure. • When the baroreceptos detect a decrease in the blood pressure, give a signal increase the sympathetic nerve activity, which cause vasoconstiction of afferent arteriole and decrease the GFR and increase blood pressure Insert fig. 17.11
Renal Autoregulation of GFR • Ability of kidney to maintain a constant GFR under systemic changes. • Achieved through effects of locally produced chemicals on the afferent arterioles. • When main arterial pressure drops to 70 mm Hg, afferent arteriole dilates. • When main arterial pressure increases, vasoconstrict afferent arterioles. • Tubuloglomerular feedback: • Increased flow of filtrate sensed by macula densa cells in thick ascending loop of henel. • Juxtaglomerular cells are cells that synthesize, store, and secrete the enzyme renin • Signals afferent arterioles to constrict.
Tubular Reabsorption All plasma constituents except the proteins are indiscriminately filtered together through the glomerular capillaries. In addition to waste products and excess materials that the body must eliminate, the filtered fluid contains nutrients, electrolytes, and other substances that the body cannot afford to lose in the urine.
Tubular reabsorption is tremendous, highly selective, and variable Tubular reabsorption is a highly selective process. All constituents except plasma proteins are at the same concentration in the glomerular filtrate as in plasma. In most cases, the quantity of each substance is the amount required to maintain the proper composition and volume of the internal fluid environment.
The essential plasma constituents regulated by the kidneys, absorptive capacity may vary depending on the body’s needs. In contrast, a large percentage of filtered waste products are present in the urine. These wastes, which are useless or even potentially harmful to the body if allowed to accumulate, are not reabsorbed to any extent.
Instead, they stay in the tubules to be eliminated in the urine. As H2O and other valuable constituents are reabsorbed, the waste products remaining in the tubular fluid become highly concentrated.
Of the 125 ml/min filtered, typically 124 ml/min are reabsorbed. Considering the magnitude of glomerular filtration, the extent of tubular reabsorption is tremendous: The tubules typically reabsorb 99% of the filtered H2O (47 gal/day), 100%of the filtered sugar (2.5 lb/day), and 99.5% of the filtered salt (0.36 lb/day).
Tubular reabsorption involvestransepithelial transport Throughout its entire length, the tubule wall is one cell thick and is in close proximity to a surrounding peritubular capillary Adjacent tubular cells do not come into contact with each other except where they are joined by tight junctions at their lateral edges near their luminal membranes, which face the tubular lumen.
Interstitial fluid lies in the gaps between adjacent cells—the lateral spaces—as well as betweenthe tubules and capillaries. The basolateral membrane faces the interstitial fluid at the base and lateral edges of the cell. The tight junctions largely prevent substances from moving between the cells, so materials must pass through the cells to leave the tubular lumen and gain entry to the blood.
An active Na+–K+ ATPase pumpin the basolateral membrane isessential for Na reabsorption Sodium reabsorption is unique and complex Of the total energy spent by the kidneys, 80% is used for Na+ transport, indicating the importance of this process. Unlike most filtered solutes, Na+ is reabsorbed throughout most of the tubule, but to varying extents in different regions. Of the Na+ filtered, 99.5% is normally reabsorbed.
Of the Na+ reabsorbed, on average 67% is reabsorbed in the proximal tubule, 25% in the loop of Henle, and 8% in the distal and collecting tubules. Sodium reabsorption plays different important roles in each of these segments.
■ Sodium reabsorption in the proximal tubule plays a pivotal role in reabsorbing glucose, amino acids, H2O, Cl-, and urea and is linked in part to K+ secretion. ■ Sodium reabsorption in the ascending limb of the loop of Henle, along with Cl- reabsorption, plays a critical role in the kidneys’ ability to produce urine of varying concentrations and volumes, depending on the body’s need to conserve or eliminate H2O.
■ Sodium reabsorption in the distal and collecting tubules is variable and subject to hormonal control. It plays a key role in regulating ECF volume, which is important in long-term control of arterial blood pressure.
Reabsorption of Salt and H20 • Return of most of the molecules and H20 from the urine filtrate back into the peritubular capillaries. • About 180 L/day of ultrafiltrate produced; however, only 1–2 L of urine excreted/24 hours. • Urine volume varies according to the needs of the body. • Minimum of 400 ml/day urine necessary to excrete metabolic wastes (obligatory water loss).
Reabsorption in Proximal Tubule Insert fig. 17.13
Proximal Convoluted Tubule • Total [solute] is = 300 mOsm/L. • Reabsorption of H20 by osmosis, cannot occur without active transport: • [Na+] in glomerular ultrafiltrate is 300 mOm/L. • Proximal convoluted tubule epithelial cells have lower [Na+]. • Due to low permeability of plasma membrane to Na+. • Active transport of Na+ out of the cell by Na+/K+ pumps. • Favors [Na+] gradient: • Na+ diffusion into cell.
Proximal Convoluted Tubule • Na+/K+ ATPase pump located in basal and lateral sides of cell membrane, creates gradient for diffusion of Na+ across the apical membrane. • Na+/K+ ATPase pump extrudes Na+. • Creates potential difference across the wall of the tubule, with lumen as –pole. • Electrical gradient causes Cl- movement towards higher [Na+]. • H20 follows by osmosis.
Salt and Water Reabsorption in Proximal Tubule Insert fig. 17.14
Significance of Proximal Convoluted Tubule Reabsorption • 65% Na+, Cl-, and H20 reabsorbed across the proximal convoluted tubule into the vascular system. • Reabsorption occurs constantly regardless of hydration state. • Not subject to hormonal regulation. • Energy expenditure is 6% of calories consumed at rest.
Countercurrent Multiplier • In order for H20 to be reabsorbed, interstitial fluid must be hypertonic. • Osmotic pressure of the interstitial tissue fluid is 4 x that of plasma. • Results partly from the fact that the tubule bends permitting interaction between the descending and ascending limbs.
Ascending Limb Loop of Henel • NaCl is actively extruded from the ascending limb into surrounding interstitial fluid. • Na+ diffuses into tubular cell with the secondary active transport of K+ and Cl-. • Occurs at a ratio of 1 Na+ and 1 K+ to 2 Cl-. Insert fig. 17.15
Ascending Limb Loop of Henel • Na+ actively transported across the basolateral membrane by Na+/ K+ ATPase pump. • Cl- passively follows Na+ down electrical gradient. • K+ passively diffuses back into filtrate. • Ascending walls are impermeable to H20. Insert fig. 17.15
Descending Limb Loop of Henel • Deeper regions of medulla reach 1400 mOsm/L. • Impermeable to passive diffusion of NaCl. • Permeable to H20. • Hypertonic interstitial fluid causes H20 movement out of the descending limb via osmosis, and H20 enters capillaries. • Fluid volume decreases in tubule, causing higher [Na+] in the ascending limb. Insert fig. 17.16