The kidneys
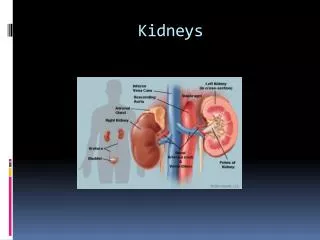
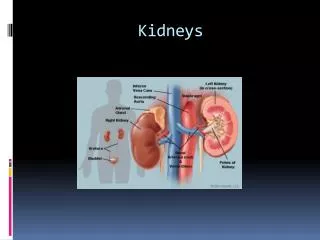
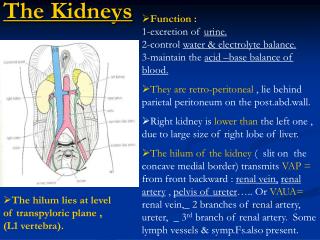
The kidneys. Location . -The kidneys are a pair of organs located in the back of the abdomen. - Each kidney is about 4 or 5 inches long -- about the size of a fist.

The kidneys
E N D
Presentation Transcript
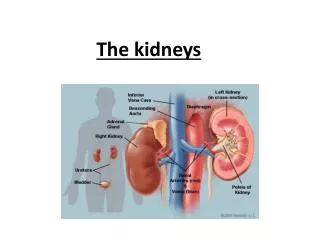
Location -The kidneys are a pair of organs located in the back of the abdomen. - Each kidney is about 4 or 5 inches long -- about the size of a fist.
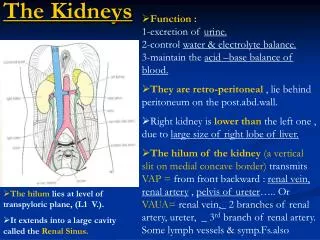
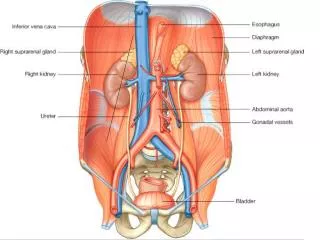
-more specifically in the paravertebral gutter and lie in a retroperitoneal position at a slightly oblique angle. There are two, one on each side of the spine -The left kidney is approximately at the vertebral level T12 to L3 and the right slightly lower. -The right kidney sits just below the diaphragm and posterior to the liver, the left below the diaphragm and posterior to thespleen.
The asymmetry within the abdominal cavity caused by the liver typically results in the right kidney being slightly lower than the left, and left kidney being located slightly more medial than the right
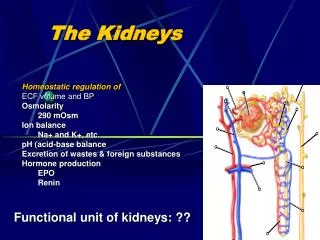
:Functions • - The kidney participates in the excretion of the body wastes • -regulating acid-base balance, • -regulating electrolyte concentrations . • -regulating extracellular fluid volume . • - regulation of blood pressure. • -Hormone secretion(including • - erythropoietin( It stimulates (production of red blood cells) in the bone marrow), • -the enzyme renin (Part of the renin-angiotensin-aldosterone system , renin is an enzyme involved in the regulation of aldosterone levels. • -Calcitriol, the activated form of vitamin D, promotes intestinal absorption of calcium and the renal reabsorption of phosphate • .
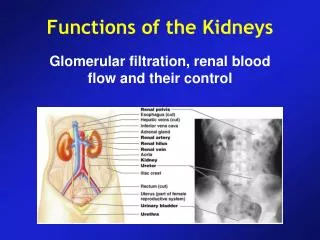
Structure and Function of the Kidney • The functional unit of the kidney is the nephron • The major functions of the kidney are to maintain extracellular fluids, to eliminate wastes resulting from normal metabolism, and to excrete xenobiotics and their metabolites • Mammalian kidneys have 10,000-1,000,000 nephrons per kidney
Structure and Function of the Kidney (cont) • The glomerulus yields an ultrafiltrate of plasma that represents 20% of the renal blood flow, ie. 2-3% of cardiac output • Endothelial surface is negatively charged and contains fenestrae • The glomerular basement membrane is sandwiched between the epithelial cells and contains anionic sialoglycoproteins, glycoproteins and collagen IV • The mesangium provides support • The outer capsule is Bowman’s capsule
Structure and Function of the Kidney (cont) • The tubule resorbs greater than 99% of the glomerular filtrate • The proximal tubule has extensive resorption and selective secretion (convoluted - S1 and S2, straight - S3). S2 is primary site for low MW protein resorption and S3 is primary site for P450. • Thin loop of Henle - resorption of fluids • Distal tubule - resorption of fluids and acid-base balance • Collecting duct - resorption of fluids, antidiuretic hormone and acid-base balance
Structure and Function of the Kidney (cont) • Produces erythropoietin, which regulates RBC production • Hydroxylates 25-OH-cholecalciferol (vitamin D metabolite), to promote bone resorption and calcium and phosphorus absorption from the gut • Releases renin to regulate the peripheral renin-angiotensin-aldosterone system (juctaglomerular apparatus)
Assessment of Kidney Function:Morphologic Evaluation • Urinalysis • Gross evaluation of the kidney at necropsy • Histopathology of the kidney • Electron microscopy of the kidney
Assessment of Kidney Function:Urinalysis • Proteinuria - indicates glomerular damage • Glycosuria - indicates tubular damage • Urine volume and osmolarity • pH • Enzymes - indicates tubular damage • Microscopic examination - casts, crystals, bacteria, etc.
Assessment of Kidney Function:Blood Chemistries • Blood urea nitrogen (BUN) • Creatinine • Electrolytes - Ca, Mg, K, P • Glomerular filtration rate - determines the clearance of inulin, creatinine and BUN • Renal clearance - measures the clearance of p-aminohippuric acid by filtration and secretion
Glomerular Disease: Toxicities due to Alteration of Anionic Charge • Hexadimethrine - polycationic molecule reduces anionic charge, which permits escape of anionic molecules such as albumin and IgG • Polynucleoside of puromycin - damages epithelial foot processes
Glomerular Disease:Immune Complex Disease • Anti-GBM mediated glomerulonephritis is induced by heterologous antibodies • Antibodies due to exogenous antigens - cationized molecules such as lysozyme, IgG and BSA bind to anionized surfaces; Concanavalin A binds to sugars in the GBM
Glomerular Disease:Immune Complex Disease (cont) Deposition of circulating immune complexes • Drug or toxin-induced T-cell dependent polyclonal B-cell activation - mercury in Brown Norway rats • Unknown mechanism - gold salts, D-penicillamine, hydralazine • Antibodies to heterologous proteins - safety evaluations of recombinant proteins in laboratory animals
Nephrosis: Damage to the renal tubule • Halogenated hydrocarbons - chloroform, hexachlorobutadiene, trichloroethylene, dibromochloropropane, & bromobenzene • Heavy metals - cadmium, mercury & lead • Antibiotics - cephalosporins & aminoglycosides • Mycotoxins - ochratoxin A & citrinin • Ethylene glycol • Antineoplastic drugs - cisplatinum • Alpha2u-globulin nephropathy
Haloalkane Nephrosis • Chloroform is metabolized by P450 to an electrophile, phosgene, which is a potent cytotoxicant. • Carbon tetrachloride is metabolized to free radicals and phosgene. • P450 is localized in the proximal tubule. • This results in nephrosis with necrosis, enzyme, glucose and protein excretion in urine, and increased BUN and creatinine concentrations in serum.
Haloalkene Nephrotoxicity • 1,1-Dichloroethylene, trichloroethylene and tetrachloroethylene are metabolized by P450 to electrophilic metabolites and or free radicals. • These metabolites can be cytotoxic and/or genotoxic. • Nephrotoxicity is exacerbated when glutathione is depleted.
Glutathione-mediated Nephrosis • Glutathione conjugates of haloalkanes can form episulfonium ions. • Primary route for 1,2-dichloroethane, 1,2-dibromoethane and 1,2-dibromo-3-chloro-propane. • These can alkylate macromolecules and cause cytotoxicity and genotoxicity.
Cystine Conjugate -lyase Activation • Stable cystine conjugates from glutathione can be formed in the liver from trichloro-ethylene, tetrafluoroethylene and hexa-chlorobutadiene and transported to the kidney. • They are further metabolized by -lyase in the kidney to generate reactive thiols.
Dialysis unit is a process for removing waste and excess water from the blood, and is used primarily to provide an artificial replacement for lost kidney function in people with renal failure Indications of dialysis in acute renal failure (ARF) -Severe fluid overload -Refractory hypertension -Uncontrollable hyperkalemia -Nausea, vomiting, poor appetite, gastritis with hemorrhage Lethargy, malaise, somnolence, stupor, coma, delirium, asterixis, tremor, seizures,
-Pericarditis (risk of hemorrhage or tamponade) -bleeding diathesis (epistaxis, gastrointestinal (GI) bleeding and etc.) -Severe metabolic acidosis - Intoxication, that is, acute poisoning with a dialysable drug, such as lithium, or aspirin. -Blood urea nitrogen (BUN) > 70 – 100 mg/dl
Indications of dialysis in chronic renal failure (CRF) -Pericarditis - Fluid overload or pulmonary edema refractory to diuretics -Accelerated hypertension poorly responsive to antihypertensives -Progressive uremic encephalopathy or neuropathy such as confusion, asterixis,-myoclonus, wrist or foot drop, seizures -Bleeding diathesis attributable to uremia
Types of Dialysis • -hemodialysis (primary) . • -peritoneal dialysis (primary) . • - hemofiltration (primary) . • - hemodiafiltration (secondary) . • - intestinal dialysis(secondary).
the patient's blood is pumped through the blood compartment of a dialyzer, exposing it to a partially permeable membrane Blood flows through the dialyzer, dialysis solution flows around the outside of the fibers, and water and wastes move between these two solutions by applying negative pressure ,The cleansed blood is then returned via the circuit back to the body
Advantages Disadvantage four dialysis-free days a week. If you travel to another country, you will have to pre-arrange access to dialysis facilities Facilities are widely available. Trained professionals are with you at all times. You can get to know other patients. You don’t have to have a partner or keep equipment in your home. your diet and the amount of fluid that you drink needs to be restricted You are advised not to drink more than a couple of cups of fluid a day You have to avoid foods that are high in potassium
In peritoneal dialysis, a sterile solution containing glucose is run through a tube into the peritoneal cavity, the abdominal body cavity around theintestine, where the peritoneal membrane acts as a partially permeable membrane The dialysate is left there for a period of time to absorb waste products, and then it is drained out through the tube and discarded. This cycle or "exchange" is normally repeated 4-5 times during the day, (sometimes more often overnight with an automated system)
Advantages Disadvantage - regular visits to a dialysis unit are not required and, in the case of home haemodialysis, there is no need to have a bulky machine installed in your house you need to perform it every day, whereas haemodialysis is usually only performed three days a week. major disadvantage of peritoneal dialysis is that your risk of developing peritonitis (infection of the peritoneum) is increased. more freedom to travel compared with haemodialysis patients. Peritonitis causes symptoms that include: abdominal pain vomiting chills (episodes of shivering and cold) fewer restrictions on diet and fluid intake compared with haemodialys reduction in protein levels, which can lead to a lack of energy and in some cases malnutrition.
Hemofiltration Hemofiltration is a similar treatment to hemodialysis, but it makes use of a different principle. The blood is pumped through a dialyzer or "hemofilter" as in dialysis, but no dialysate is used. - A pressure gradient is applied; as a result, water moves across the very permeable membrane rapidly, "dragging" along with it many dissolved substances, including ones with large molecular weights, which are not cleared as well by hemodialysis. Salts and water lost from the blood during this process are replaced with a "substitution fluid" that is infused into the extracorporeal circuit during the treatment.
Hemodiafiltration Hemodiafiltration is a term used to describe several methods of combining hemodialysis and hemofiltration in one process.
Intestinal dialysis In intestinal dialysis, the diet is supplemented with soluble fibres such as acacia fibre, which is digested by bacteria in the colon. This bacterial growth increases the amount of nitrogen that is eliminated in fecal waste An alternative approach utilizes the ingestion of 1 to 1.5 liters of non-absorbable solutions of polyethylene glycol or mannitol every fourth hour.
Electric cardioversion a medical procedure by which an abnormally fast heart rate or cardiac arrhythmia is converted to a normal rhythm, using electricity
The purpose of the cardioversion is to interrupt the abnormal electrical circuit(s) in the heart and to restore a normal heartbeat. The delivered shock causes all the heart cells to contract simultaneously, thereby interrupting and terminating the abnormal electrical rhythm (typically fibrillation of the atria) without damaging the heart.
two electrode pads are used These are connected by cables to a machine which has the combined functions of an ECG display screen and the electrical function of a defibrillator Indications: • - Synchronized electrical cardioversion is used to treat hemodynamically significant supraventriculartachycardias, including atrial fibrillation and atrial flutter. It is also used in the emergent treatment including ventricular tachycardia, when a pulse is present. • -Pulselessventricular tachycardia and ventricular fibrillation are treated with unsynchronized shocks referred to as defibrillation.
Ventialtor a machine designed to mechanically move breatheable air into and out of the lungs, to provide the mechanism of breathing for a patient who is physically unable to breathe, or breathing insufficiently.
Indications : -Acute lung injury (including ARDS, trauma) - Apnea with respiratory arrest, including cases from intoxication -Chronic obstructive pulmonary disease (COPD) -Acute respiratory acidosis with partial pressure of carbon dioxide (pCO2) > 50 mmHg and pH < 7.25, which may be due to paralysis of the diaphragm due to Guillain-Barrésyndrome,Myasthenia Gravis, spinal cord injury, or the effect of anaesthetic and muscle relaxant drugs -Increased work of breathing as evidenced by significant tachypnea, retractions, and other physical signs of respiratory distress Lateral Sclerosis
-Hypoxemia with arterial partial pressure of oxygen (PaO2) < 55 mm Hg with supplemental fraction of inspired oxygen (FiO2) = 1.0 -Hypotension including sepsis, shock, congestive heart failure Neurological diseases such as Muscular Dystrophy and Amyotrophic
Disadvantages: It carries many potential complications including pneumothorax, airway injury, alveolar damage, and ventilator-associated pneumonia. It is used to support a single failing organ system (the lungs) and cannot reverse any underlying disease process (such as terminal cancer)
Cardiac Assist Devices Wayne E. Ellis, Ph.D., CRNA
Types Pacemakers AICDs VADs
History • First pacemaker implanted in 1958 • First ICD implanted in 1980 • Greater than 500,000 patients in the US population have pacemakers • 115,000 implanted each year
Pacemakers Today • Single or dual chamber • Multiple programmable features • Adaptive rate pacing • Programmable lead configuration
Internal Cardiac Defibrillators (ICD) • Transvenous leads • Multiprogrammable • Incorporate all capabilities of contemporary pacemakers • Storage capacity
Temporary Pacing Indications • Routes = Transvenous, transcutaneous, esophageal • Unstable bradydysrhythmias • Atrioventricular heart block • Unstable tachydysrhythmias • *Endpoint reached after resolution of the problem or permanent pacemaker implantation