Download
1 / 1
20 likes | 223 Vues
Z Score Neurofeedback (NFB) for Insomnia Barbara U. Hammer, PhD 1 , Agatha P. Colbert, MD 1 Kimberly A. Brown, MSOM 1 , Elena C. Ilioi 2 , 1 Helfgott Research Institute, National College of Natural Medicine (NCNM), Portland, OR; 2 McGill University, Montreal, Quebec, Canada. Abstract

E N D
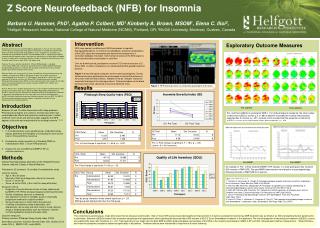
Z Score Neurofeedback (NFB) for Insomnia Barbara U. Hammer, PhD1, Agatha P. Colbert, MD1 Kimberly A. Brown, MSOM1, Elena C. Ilioi2, 1Helfgott Research Institute, National College of Natural Medicine (NCNM), Portland, OR; 2McGill University, Montreal, Quebec, Canada • Abstract • Background: Insomnia has reached epidemic proportions in the US. The most widely used treatments are pharmaceutical agents that may be associated with negative side effects and when discontinued sleep problems return. Insomnia has the highest co-morbidity with psychological disorders. Neurofeedback (NFB) is a psycho-physiological treatment without reported serious side effect, the effectiveness of which does not appear to diminish rapidly after treatment completion. Despite its demonstrated effectiveness for insomnia almost 30 years ago, NFB is not widely used. • Purpose: To assess whether two distinct Z Score NFB protocols, a standard sensorimotor (SMR) and a sequential, quantitative EEG (sQEEG) guided Individually Designed (IND) protocol, can alleviate the disturbed sleep behavior and associated daytime dysfunctions of adults with insomnia. • Methods: Adults with Insomnia (N=12) were recruited from the general community and randomly assigned to the SMR or IND group. All were free of other mental and (uncontrolled) physical disorders; 8/12 participants completed the study. Each group received 15 20-minute sessions of Z-Score NFB. Outcome measures included: Pittsburgh Sleep Quality Index (PSQI), Insomnia Severity Index (ISI), Quality of Life Index (QOLI), Minnesota Multiphasic Personality Inventory, (MMPI-2-RF), QEEG, and Actigraphy and sQeeg. • Results: Paired t-tests yielded significant pre versus post treatment improvement for both groups on all Insomnia total scores (PSQI=p<.0001, ISI=p<.005),Sleep Efficiency (p<.007), and QOLI (p<.02). Binomial tests of baseline EEGs of all participants indicated a significantly high proportion of excessively high levels of Delta and Beta power (p<.001)that were significantly lower post-treatment (paired z-tests p<.001). On MMPI-2-RF, pre-treatment borderline-normal subjects showed post-treatment clinical improvement with normalized profiles. • Introduction • Between 40 and 70 million Americans suffer sleep problems. Pharmaceutical agents are useful for Insomnia but often have undesirable side effects and cannot be used long term. Limited evidence from human and animal studies suggests that NFB appears to be safe and may beneficial for treating Insomnia.1,2,3,45 • Objectives • In a randomized pre- post, parallel group, single blind study design, determine the feasibility of conducting a future clinical trial of Z Score NFB for Insomnia. • Evaluate the relative benefits of a Standard (SMR) vs. Individualized (IND) Z Score NFB protocols. • Explore the use of sQEEG and MMPI-2 RF as outcome measures. • Methods • Setting: Psychophysiology laboratory at the Helfgott Research Institute, National College of Natural Medicine • Participants: 25 screened, 12 enrolled, 8 completed the study • Inclusion criteria: • Age ≥ 18 to 65 years • Meet all of Roth et al diagnostic criteria for Insomnia: • Score >7 on the ISI • Score >8 on the PSQI (>5 is cutoff for sleep difficulties) • Exclusion criteria: • Diagnosis of mental disorder at time of study (determined by MMPI-2 RF, PDSQ and psychological screening interview). • History of epilepsy, seizures, or dementia • Any significant, severe or unstable, acute or chronically progressive medical or surgical condition • Serious head injury or stroke within the past year • Unwilling to discontinue sleep medications, anti- depressants, anti-anxiety and other mind or mood- altering drugs or herbal preparations such as melatonin, valerian root and tryptophan during the 8-week study. • Outcome measures: • Primary outcome: Pittsburgh Sleep Quality Index (PSQI) • Secondary outcomes: Insomnia Severity Index (ISI), Quality of Life Index (QOLI), (MMPI-2-RF), and sQEEG. Intervention NFB uses operant conditioning of EEG brainwaves to regulate dysregulated patterns. In Z Score neurofeedback, statistical computations of the EEG signal are instantaneously derived and compared to a normative database. Deviation from normal (Z score) of the EEG signal is then trained toward normaliization in real time. Over an 8-week period, participants received 15 20-minute sessions of Z-Score NFB in either a standard or an individualized EEG-guided treatment protocol. Figure 1 shows the typical computer screen seen by participants. During treatment sessions participants are encouraged to control the pictures on the screen with their brain waves. Marbles in the jar indicate reward for successful learning of the training protocol. Colored numbers on the black training screen show abnormal Z scores at identified sites. Exploratory Outcome Measures Figure 1: NFB training screen as viewed by participant and trainer. Results Pre-sQEEG Post-sQEEG Pre- and Post-sQEEGs in participant SMR-1. For all 8 participants combined, the total number of abnormal sQEEG z-scores (z ≥ ±1.96) at baseline exceeded the number that would be expected due to chance, p< .001. A paired z-test revealed that the proportion of abnormal sQEEG z-scores was significantly lower after treatment, p< .001. Pre- to Post-change is significant, F = 18.2, p < .005 (score < 8 = No Insomnia). Pre- to Post-change is significant, F = 55.6, p < .0001. Pre-MMPI Post-MMPI Pre- Post-change is significant, F= 9.6, p < .02. An example of Pre- to Post-treatment MMPI 2-RF change in a male participant who received 260 minutes of SMR NFB. The post-MMPI demonstrates normalization of psychopathology following 8 weeks of SMR NFB for insomnia. Abreviated Reference List: 1. Cortoos A, Verstraeten E, Cluydts R. Neurophysiological aspects of primary insomnia: implications for its treatment. Sleep Med Rev 2006;10(4):255-66. 2. Sterman MB, Howe RC, Macdonald LR. Facilitation of spindle-burst sleep by conditioning of electroencephalographic activity while awake. Science 1970;167(921):1146-8. 3. Roth SR, Sterman MB, Clemente CD. Comparison of EEG correlates of reinforcement, internal inhibition and sleep. Electroencephalogr Clin Neurophysiol 1967;23(6):509-20. 4. Hauri P. Treating psychophysiologic insomnia with biofeedback. Arch Gen Psychiatry 1981;38(7):752-8. 5. Hauri PJ, Percy L, Hellekson C, Hartmann E, Russ D. The treatment of psychophysiologic insomnia with biofeedback: a replication study. Biofeedback Self Regul 1982;7(2):223-35. Insert description here Time by group interaction tends toward significant, p < .23. SMR group did slightly better then the IND group. • Conclusions • This randomized, parallel-group, single-blind experimental design proved feasible. Both Z Score NFB protocols provided significant improvement in Insomnia and daytime functioning. SMR treatment was as effective as IND and significantly less burdensome to administer. Baseline sQEEGs showed both excessive sleepiness and hyperarousal, which significantly improved after ≤300 minutes of EEG Z Score Biofeedback treatment in the laboratory. The overall proportion of abnormal pre-treatment sQEEG z-scores was significantly lower after treatment, p < .001. Training at two to four scalpsites (for both SMR and IND) produced global normalization of the EEG in the majority of participants. MMPI-2-RF and QOLI showed post-treatment improvement. Sleep Efficiency and Insomnia symptoms/complaints improved significantly in all patients. Treatment effects were maintained or improved at 6 month follow-up.