How We Zapped VAP
How We Zapped VAP. During the past six years, our Multidisciplinary Pneumonia Team has worked to reduce Ventilator Associated Pneumonia (VAP ). Through these efforts, our facility has reported zero VAPs within the last 58 months (May 08-Present).

How We Zapped VAP
E N D
Presentation Transcript
How We Zapped VAP • During the past six years, our Multidisciplinary Pneumonia Team has worked to reduce Ventilator Associated Pneumonia (VAP). • Through these efforts, our facility has reported zero VAPs within the last 58 months (May 08-Present). • Our multidisciplinary pneumonia team explored evidence-based research through the Georgia Hospital Association (GHA), Partnership for Health and Accountability (PHA), National Health and Safety Network (NHSN), and the Institute of Healthcare Improvement (IHI) 5million Lives Campaign to determine best practice approaches. • Armed with this information, our organization implemented a ventilator bundle incorporating the following criteria listed in the next section.
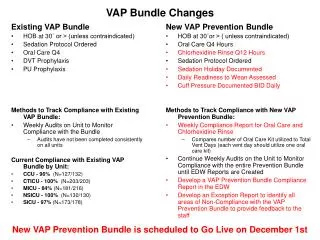
Objectives To achieve compliance with the VAP bundle: • elevate the head of bed to 30 degrees • conduct daily awakening and assess readiness to extubate • ensure peptic ulcer disease prophylaxis • ensure deep vein thrombosis prophylaxis • oral care with CHG (chlorohexidine) twice a day (Purple Packs)
Process Process: Bundle implemented in 2006. With numerous revisions due to changes in evidence based practice guidelines and our internal findings. • Latest update included the addition of the daily readiness to extubate assessment in ’09 and adding sacral dressing to minimize the shirring effect on the skin due to the elevated HOB. • Also in ‘09 we added the Critical Care Sedation Physician Order set for the ventilated patient.
PDCA • Plan • Multidisciplinary team approach to create the Vent bundle. The team included an intensivist/ pulmonologist, pharmacy, respiratory therapy, IT, physical therapy, dietician, wound therapy, and critical care RN. • 2006 we launched our efforts to eradicate VAP in our healthcare system. Focusing on ICU and NCCU • With the 5 key elements listed in our bundle/order-set it quickly passed through all approval process (Critical Care Committee, Quality Committee, Medical Executive Committee, and Senior Leadership.
PDCA • Do • It took a team to develop the Vent bundle which was implemented in early ‘07. • Many changes were made to keep up with best practice guidelines as well as fixing what was not working with in out process. • Ultimately the end result encompassed all objectives that were checked for compliance.
PDCA • Check/Study • Each bundle element was studied to look for challenges in compliance
PDCA • Check/Study • Each bundle element was studied to look for challenges in compliance • After compliance with HOB was 100% for so long we considered this a culture change and no longer kept the data.
PDCA • Check/Study • Each bundle element was studied to look for challenges in compliance • VTE data will most likely drop off after this quarter as we have met 100% for 14 qtrs.
PDCA • Check/Study-Multidisciplinary Rounding
PDCA • Check/Study-Readiness to Wean • Obstacle: was the readiness to wean process. These orders were not part of the original bundle and we did not have a standardized sedation order set • During the implementation of the sedation protocol, we discovered that the readiness to wean assessment on the respiratory documentation tool was lacking key information. In working with the clinical informatics department, a new and improved assessment tool was implemented. The Critical Care Sedation Order Set now guides the practitioners through the daily weaning process.
Daily Awakening • Hold/stop sedation at 0800 • Assess patient’s sedation level • Perform weaning mechanics or chart contraindications • If awakening is tolerated and continued sedation is needed RESTART infusion at 50% previous rate (if sedation regimen has been longer than 5 days reduce rate by 20% and monitor for withdrawal) • If daily awakening NOT performed MUST document rational on daily rounds sheet.
PDCA • Check/Study-Readiness to Wean
PDCA • Act-Lessons learned for future improvement • Ensure oral care and documentation completed every two hour • Ensure placement of the Critical Care Sedation Protocols on each patient’s chart that is on a ventilator • Educate in the readiness to wean guidelines and encourage proper respiratory therapy documentation • Reinforce sedation agitation education and documentation every hour • Monitor daily awakening and evaluate patients at risk for self extubation