Cardiovascular Physiology
Cardiovascular Physiology. Dr. Abdulhalim Serafi, MB ChB,MSc,PhD,FESC Assistant Professor & Consultant Cardiologist Faculty of Medicine and Medical Sciences Umm Al-Qura University Makkah Al-Mukarramah Saudi Arabia. Part II CARDIOVASCULAR PHYSIOLOGY.

Cardiovascular Physiology
E N D
Presentation Transcript
Cardiovascular Physiology Dr. Abdulhalim Serafi, MB ChB,MSc,PhD,FESC Assistant Professor & Consultant Cardiologist Faculty of Medicine and Medical Sciences Umm Al-Qura University Makkah Al-Mukarramah Saudi Arabia
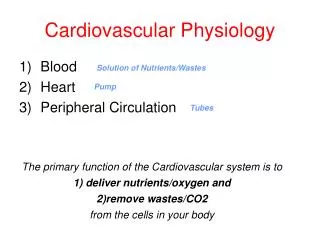
Part II CARDIOVASCULAR PHYSIOLOGY LECTURE II:ARTERIAL BLOOD PRESSURE (ABP) • Outline: • - Systolic BP and diastolic BP. • - Pulse pressure and mean ABP. • - Physiological variations of ABP. • - Factors that maintain normal ABP: • : Cardiac output (co) • : Peripheral resistance (PR) • : Arterial elasticity • : Blood volume • Further Reading: • Guyton: Textbook of Medical Physiology • Ganong: Review of Medical Physiology
ARTERIAL BLOOD PRESSURE (ABP) • Arterial Blood Pressure (ABP) is the lateral pressure exerted by the blood on the arterial walls. It oscillates during each cardiac cycle between a maximum called systolic BP and a minimum called diastolic BP. • Systolic BP: • It is the maximal pressure exerted by the blood on the arterial walls during ventricular systole (ejection of blood from the left ventricle into the aorta). • It ranges between 95 and 145 mm Hg with an average of about 120 mm Hg in adults i.e. normal systolic BP=120 ± 25. Mm Hg. • Diastolic BP: • It is the minimal pressure exerted by the blood on the arterial walls during ventricular diastole (just before ventricular systole and ejection of blood)
Pulse pressure: • It is the difference between systolic blood pressure and diastolic blood pressure e.g. PP=120-80 = 40 mm Hg. • Mean Arterial BP: • It is the average pressure in the arteries throughout cardiac cycle. • It is calculated by the following formula: • Mean arterial BP = Diastolic BP + 1/3 Pulse Pressure e.g. • = 80 + 1/3 x 40 = about 93 • mm Hg.
IMPORTANCE OF ABP • Normal mean ABP provides the force that drives blood to the tissues I.e. ensures steady blood flow (perfusion) to the tissues. • Normal diastolic blood pressure is needed for filling of the coronary arteries with blood which occurs mainly during ventricular diastole. • PHYSIOLOGICAL VARIATIONS IN ABP: • AGE: • - At birth, the ABP is about 80/40 • - At the age of 120 years, the ABP is about 120/ 80 • - The ABP tends to increase with age e.g. it becomes about 150/90 at the age of 60 years.
SEX: • - The ABP is slightly higher in adult males than adult females • - After menopause (stoppage of menstrual cycle in females which occurs usually at the of 45 years), the ABP may be the same in females and males, but sometimes it becomes higher in females, probably due to hormonal change. • (3) Body Built: • - The ABP of obese persons is usually higher than that of persons with normal body weight. • - Also, obese persons have higher tendency to develop hypertension. • (4) Exercise: • - the ABP (systolic BP) increases during muscular exercise (due to increase of cardiac output) but it drops to pre-exercise level during recovery.
- the diastolic BP may remain unchanged or it id slightly decreased due to vasodilatation of the arterioles of the active skeletal muscles. • (5) Emotions: • - ABP (mainly systolic) increases during emotions due to sympathetic over activity. • (6) Meals: • - ABP rises slightly after meals. • (7) Sleep: • - ABP decreases slightly during sleep. • - When sleep is accompanied with dreams (nightmares) of emotional or motor activity, the ABP may increase to high levels.
CONTROL OF ABP Factors that determine and maintain ABP • Cardiac output. • Peripheral resistance • Arterial elasticity • Blood volume • ABP is related to the cardiac output and peripheral resistance according to the following equation: • ABP = Cardiac output x Peripheral resistance
Cardiac Output (COP) • Normal COP is essential for normal ABP. • ABP is directly proportional to COP (provided that all other factors affecting ABP remain constant). • Change in COP affects systolic BP more than diastolic BP. • COP = Heart rate x Stroke volume • Effect of change in stroke volume: • Changes in SV affect systolic BP more than diastolic BP. Thus, SV systolic BP & SV systolic BP. • The diastolic BP shows little or no change. • Effect of change in heart rate: • Changes in HR affect diastolic more than systolic BP i.e. heart rate of diastolic BP & HR of diastolic BP. • Systolic BP shows little or no change.
Peripheral resistance (PR) • PR is the resistance which blood meets during its passage in the peripheral arterioles and to a smaller extent in the blood capillaries. • ABP is directly proportional to PR. Changes in the peripheral resistance affect diastolic BP more than systolic BP. • The PR depends mainly on 2 factors: (diameter of arterioles and blood viscosity) • Diameter of arterioles: • - The PR is inversely proportional to the diameter of arterioles i.e. • Vasoconstriction of arterioles of their diameter PR ABP (manly diastolic)
Vasodilatation of arterioles of their diameter PR ABP (mainly diastolic) • Blood Viscosity: • PR is directly proportional to the blood viscosity. • Blood viscosity depends on 2 factors • HV (haematocrit value) • Plasma proteins • Blood viscosity as in polycythaemia PR ABP • blood viscosity as in severe anemia or hypoproteinaemia PR ABP
Factors that determine the peripheral resistance • The peripheral resistance (PR) is essential for maintenance • of the arterial B.P. (particularly the diastolic B.P.). It occurs • mainly in the arterioles and is determined by the following • factors: • 1. Radius (r) of the blood vessel: The PR varies inversely with the fourth power of the radius (i.e. PR I/r4). • Blood viscosity (V): This is determined mainly by the • haematocrit value and to a lesser extent by the • plasma proteins. The PR varies directly with the blood viscosity (i.e. PR V). • 3. Length (L) of the blood vessel: The PR varies directly with the length of the blood vessel (i.e. PR L) However, the radius is the most important factor that determines the PR because both V and L are normally • constant.
Effect of peripheral resistance • (PR) on ABP • PR = resistance which the blood meets during its passage in the peripheral arterioles and to a smaller extent in the blood capillaries. • Changes in PR affect diastolic BP more than systolic BP • PR depends mainly on 2 factors: • Diameter of arterioles: - VC of arterioles PR ABP - VD of arterioles PR ABP • Blood viscosity - Blood viscosity PR ABP - Blood viscosity PR ABP
Regulation of the diameter of the arterioles • (=Nervous & chemical regulation) • Nervous Regulation • The diameter of arteriole is under the control of the vaso-motor center (VMC) present in the medulla oblongata and the VC sympathetic tone (from VMC) to the arterioles) • The activity of the VMC is modified by impulses from the arterial baroreceptors, chemoreceptors, atrial receptors and other receptors e.g. in skeletal and skin • Chemical Regulation • The arterioles show VD or VC by some chemical or hormonal agents. • Vasoconstrictor substance e.g. noradrenalin, vasopressin (ADH) & angiotensin II
Vasodilator substances e.g. metabolites, acetylcholine, histamine and bradykinine. • The diameter of arterioles is regulated by 2 mechanisms (nervous and chemical): • Nervous regulation: • The diameter of arterioles is under the control of the vasomotor center (VMC) which is present in the medulla oblongata. • The VMC discharges continuous vasoconstrictor impulses through sympathetic nerve fibers to the various arterioles to keep them in a state of moderate or partial vasoconstriction. This is called vasomotor tone and it is important to maintain normal ABP.
The activity of the VMC (:: sympathetic vasomotor tone) is modified impulses from the arterial baroreceptors, the peripheral chemoreceptors, atrial receptors and other receptors e.g. in skeletal muscles and skin. vasomotor tone more constriction of the arterioles PR ABP vasomotor tone less constriction of the arterioles VD PR ABP • Chemical regulation: - The arterioles show VC or VD by some chemical or hormonal agents: Vasoconstrictor substance: e.g. noradrenalin, vasopressin (ADH) angiotensin II.
Vasoconstrictor substance: e.g. metabolites, acetylcholine, histamine and bradykinine. • Elasticity of the arterial walls: The elasticity of the wall of the aorta and its large branches buffers excessive changes in ABP during each cardiac cycle; • During ventricular systole The aorta distends and its capacity is increased to accommodate for the ejected blood pressure from the left ventricle. This prevents the systolic BP from reaching high level.
During ventricular diastole The aorta recoils and its capacity is decreased. This prevents the diastolic BP from reaching a low level. Therefore, elastic recoil of the arterial wall is important for maintenance of normal diastolic BP. The elastic recoil of the arterial wall is also useful in pushing the blood towards the tissues during diastole. • In arterioscleroses The arterial elasticity is decreased systolic BP diastolic BP.
Normal diastolic BPis produced and maintained by: • Elastic recoil of aorta and large arteries. • Normal degree of peripheral resistance. Normal diastolic BPis important for: • Filling of the coronary arteries which occurs mainly during ventricular diastole. • Maintenance of blood flow to the tissues during ventricular diastole
Blood volume: Normal blood volume (5-6 liters with normal vascular capacity) is important for normal ABP (systolic and diastolic) Slight or moderate change in the blood volume almost no effect on ABP due to some compensatory reaction in the CVS that restore normal BP e.g. Moderate of blood volume baroreceptors reflex heart rate and vasoconstriction of arterioles ABP towards normal.
Marked or excessive decrease of blood volume e.g. after severe haemorrhage decrease of ABP (hypotension as hemorrhagic shock). This occurs because the compensatory reactions are not sufficient to restore normal BP. Decrease of the circulatory capacity (with normal blood volume) ABP e.g. injection of noradrenalin generalized vasoconstriction of the circulatory capacity ABP. Increase of the circulatory capacity (with normal blood volume) ABP e.g. injection of histamine (in experimental animals) generalized vasodilatation circulatory capacity ABP (=histamine shock).
Regulation (control) of the blood volume includes the • following: • Red cell volume is kept constant by a balance between • the rate of destruction & regeneration of RBCs • Plasma volume is kept constant by: • Rapid mechanism = interchange of fluid between plasma and the tissue fluid. • Slow mechanism = balance between water loss and water gain. • Water excretion in urine is controlled by 2 hormones. • Antidiuretic hormone (ADH) secreted by the posterior pituitary. • Aldosterone secreted by the supra renal cortex. • These hormones regulate the blood volume through their • effects on the kidney (urine formation). Long-term regulation of the ABP.
Part II CARDIOVASCULAR PHYSIOLOGY LECTURE III:REGULATION OF ARTERIAL BP • Outline: • - Short-term regulation of the ABP. • : Nervous mechanisms e.g. baroreceptors reflexes. • : Hormonal mechanisms e.g. epinephrine – • nor epinephrine. • : Capillary fluid shift mechanism. • - Long-term regulation of the ABP. • : Renal-body fluid – pressure control mechanism • - Hypertension (definition, types & causes). • Further Reading: • Guyton: Textbook of Medical Physiology • Ganong: Review of Medical Physiology
CONTROL OF ABP • The normal mean ABP ensures a steady blood flow or perfusion to the tissues, particularly the vital organs e.g. brain and heart. Regulation of mean ABP includes: • Short-term regulation. • Long-term regulation. • I-Short-term regulation of the ABP: • This includes the following rapidly-acting pressure control mechanisms: • Nervous mechanisms for rapid control of ABP e.g.: • Baroreceptors reflexes (=arterial baroreceptors reflex mechanisms): • = Feed-back control system that prevents sudden or • of ABP e.g.
ABP reflex of heart rate + reflex vasodilatation of arterioles ABP. • ABP reflex of heart rate + reflex vasodilatation of arterioles ABP. • Chemoreceptor reflexes: • ABP (as in haemorrhage) blood flow to the peripheral chemoreceptors hypoxia of these receptors ( PO2) reflex of heart rate + reflex vasoconstriction of the arterioles ABP. • Atrial reflexes: • blood volume venous return (VR) stretch of the right atrium stimulation of stretch (volume) receptors reflex venodilation venous capacity venous return.
N.B. (1) ARTERIAL BAROREFLEXES: An acute rise on arterial blood pressure produces reflex: • Decrease in heart rate. • Peripheral vasodilatation (specially the blood vessels of the skeletal muscles). A fall in ABP produces the opposite reflex effects, i.e. increase in the heart rate and vasoconstriction.
The reflex pathway: Receptors : Baroreceptors in the carotid sinus & aortic arch Afferents : The carotid sinus branch of the glassopharyngeal nerve, and the aortic branch of the vagus nerve Center : The medullar cardiovascular centers Efferent : The vagal and sympathetic cardiac nerves and sympathetic nerves to the blood vessels. Effected organs : The heart and blood vessels. These reflexes correct a rise in pressure by decreasing the cardiac pumping (decrease in heart rate) and the peripheral resistance (vasodilatation). The opposite effects occur if the ABP falls. In this way, these reflexes maintain the normal level of ABP
The arterial baroreflexes are very rapid. They start in less than one second. They are quite powerful reflexes. They play a very important role to prevents reflexes correct a rise in pressure by decreasing the cardiac pumping (decrease in heart rate) and the peripheral resistance (vasodilatation). The opposite effects occur if the ABP falls. In this way, these reflexes maintain the normal level of ABP.
N.B. (2) THE CNS ISCHEMIC RESPONSE: Ischemia of the CNS produces powerful generalized vasoconstriction and elevation of ABP. This response is very important in cases of severe hypotension, at blood pressures below 60 mm Hg. Hypotension reduces the blood flow to the brain (ischemia). In the medulla, ischemia produces local hypoxia, hypercapnia and acidosis which are strong stimulants of the medullar vasoconstrictor center. The severe vasoconstriction elevates the ABP toward normal to improve the blood flow to the brain.
Hormonal mechanisms for rapid control of ABP e.g: • Epinephrine-nor epinephrine mechanism: - ABP a baroreceptors reflex sympathetic stimulation secretion of epinephrine and nor epinephrine from the suprarenal medulla. - Epinephrine causes HR & nor epinephrine causes strong VC ABP. • Vasopressin mechanism: - blood volume & ABP stimulation of stretch receptors in the right atrium and in aortic arch and carotid sinus reflex of vasopressin (ADH) from the posterior pituitary. Vasopressin urine vol. & vasoconstriction. ABP.
c) Renin-angiotensin-aldosterone mechanism: • ABP renal ischemia release of a chemical substance called rennin from the juxtaglomerular cells (JGC) of the kidney. • Renin acts as a proteolytic enzyme which acts on a plasma 2 – globulin formed by the liver called angiotensinogen and converts it into decapeptide called angiotensin I (AI). • Angiotensin I (AI) is converted into octapeptide called angiotensin II (AII) by angiotensin converting enzyme (ACE) mainly in the lungs. • Angiotensin II (AII) ABP by two mechanisms: 1) AII is a powerful vasoconstrictor generalized vasoconstriction peripheral resistance ABP.
2) A II stimulates the secretion of Aldosterone hormone from the suprarenal cortex. Aldosterone causes Na & H2O reabsorption from renal tubules salt and water retention blood volume ABP. 3) Capillary fluid shift mechanism for rapid control of ABP: - The interstitial fluid acts as a reservoir for the plasma i.e for regulation of blood volume, and in turn, regulation of ABP. - ABP filtration (=fluid shift) from the capillaries to the interstitial fluid (tissue fluid) ABP. - ABP filtration & reabsorption (fluid shift) from the interstitial fluid into the capillaries blood volume ABP.
Long-term regulation of the ABP: This is a slowly-acting pressure control mechanism called “renal-body fluid-pressure control mechanism”. It includes the hormonal mechanism which acts through the kidney • Regulation of extra-cellular fluid (blood volume with its effects on ABP) • Excretion of water and electrolytes in urine. Two hormones are involved in this mechanism: • Anti diuretic hormone (ADH) which is secreted from the posterior pituitary and it helps H2O reabsorption from the renal tubules blood volume. • Aldosterone hormone which is secreted from the suprarenal cortex and it helps Na+ and H2O reabsorption from the renal tubules blood volume
Summary REGULATION OF THE ABP Short-term regulationLong-term regulation = Rapidly-acting pressure = Slowly-acting pressure control mechanism. control mechanism. Includes: Includes: a) Nervous mechanisms e.g.: Hormonal mechanism which - baroreceptors reflexes. acts through the kidney - Chemoreceptor reflexes. Regulation of extra cellular - Atrial reflexes. fluid (blood volume with effects on ABP).
b) Hormonal mechanisms e.g.: • - Epinephrine nor Excretion of water & • epinephrine secretion electrolytes in urine • - ADH (vasopressin) Hormones which affect • secretion urine formation (volume) • - Renin-angiostensin - ADH (vasopressin). • mechanism - Aldosterone • c) Capillary fluid shift Long-term regulation=renal • mechanisms: - body fluid-pressure • - Shift of fluid from capillaries control mechanism. • into the interstitial fluid. • - Shift of fluid from the interstitial • fluid into the blood capillaries.
HYPERTENSION - Hypertension is diagnosed when the arterial BP exceeds • 150/95 (in adults 20-50 years) on repeated estimation. It • may be one of the following types: • 1- Primary (essential) hypertension: This occurs as a result • of arteriolar vasoconstriction. The exact cause is • unknown. • 2- Secondary hypertension: This occurs as a result of • another disease e.g. secondary to a tumor in the supra- • renal gland secretion of cortisol, Aldosterone & • adrenaline. • 3- Malignant hypertension: This is a severe type • characterized by marked elevation of ABP without obvious • causes.
EXPERIMENTAL HYPERTENSION - Hypertension is a sustained elevation of ABP. Hypertension can be produced in experimental animals by the following methods: • 1- Renal ischemia (interference with renal blood flow). • 2- Denervation of vaso-sensory area (aortic arch and carotid • sinus). • 3- Experimental neurosis by efferent stimuli such as loud • noises. • 4- Chronic injection of supra-renal cortical hormones. • Experimental hypertension is of great value in study in the • possible causes of hypertension in man and the effect of • drugs on hypertension.
Hypertension is a chronic state of • elevated arterial blood pressure: • The upper limits of normal ABP in different age groups Any levels higher than these limits are considered as hypertension
Renal ischemia and ABP: • Unilateral renal ischemia temporary hypertension because the healthy kidney (which is not ischaemic) produces angiotensinase enzyme which inactivates angiotensin II • Bilateral renal ischemia permanent hypertension. N.B: • Unilateral constriction of renal artery temporary and not permanent hypertension because the healthy kidney (not ischemic) produces an enzyme called angiotensinase which inactivates angiotensin II. • ABP, blood volume, body sodium release of rennin activation of rennin – angiotensin system.