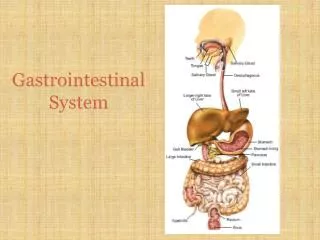
Gastrointestinal system
Gastrointestinal system. By S.S Eghbali,MD,ApCp Bushehr 2009. Gastrointestinal pathology Part I. Mouth and oral cavity. The mouth. Teeth (caries) Action of Streptococci on dietary sugars Leads to pulpitis and abscess. Oral mucosa. Squamous epithelium

Gastrointestinal system
E N D
Presentation Transcript
Gastrointestinal system By S.S Eghbali,MD,ApCp Bushehr 2009
Gastrointestinal pathology Part I • Mouth and oral cavity
The mouth • Teeth (caries) • Action of Streptococci on dietary sugars • Leads to pulpitis and abscess
Oral mucosa • Squamous epithelium • Subject to infection • Herpes virus • Candida • Hairy leukoplakia (HIV associated – caused by EBV)
Premalignant lesions • Leukoplakia • Erythroplakia
Leukoplakia • Tubacco • Hpv infection • Chronic irritation • Alcohole • Special diets • Hyperkeratosis with or without dysplasia • Progress to Invasive scc upto 5-15%
Erythroplakia • Red &granular lesions • Severe dysplasia • Progress to invasive scc >50%
Oral cancers • <3% all visceral malignancies • Age >60 • Fatality>50% SCC is the most common type • Common sites: lip,palate,tongue • Lymphatic metas.: 50-60%
Oral cancer • Associated with tobacco (chewing) and alcohol • Clinical preinvasive lesion (leukoplakia) • Squamous carcinoma • Poor prognosis unless detected early
Salivary glands • Sialadenitis& sialolithiasis • Viral sialadenitis(mumps) • Bacterial sialadenitis • Dry mouth • Sialolithiasis(calculi) • Medical and surgical treatment
Autoimmune sialadenitis(Sjogrene syndrome) • Xerostomia • Keratoconjunctivitis(Sicca) • Sialoadenitis(painless swealing ) • Primary& secondary(lymphoma,leukemia,sarco-idosis,…)
Histopathology findings • Intrestitial Edema • Mono nuclear infiltration • Cell necrosis(bacterial infections)
Salivary tumours • Benign: • Pleomorphic adenoma • Warthin’s tumour • Malignant: • Muco-epidermoid tumour • Adenoid cystic carcinoma • Adenocarcinoma
Tumours • In the bigger glands most tumours are benign • More often malignant in minor salivary glands
Pleomorphic adenoma(Benign mixed tumor) • Most common salivary tumor • Slow growing • Encapsulated • Fascial nerve • Recurance>10% • Malig.transformation 15-40% • Bimodal Pattern • Glandular comp. • Stomal comp. • Origin: myoepithelial
Pleomorphic adenoma • Most common salivary tumour • Mucoid “cartilagenous” stroma with epithelial proliferation • Prone to local recurrence
Warthins tumor(papillary cystadenoma ,Cystadenolymphoma) • Common site: parotid • Encapsulated • Cyst&cleft • Benign with >10% recurrance • No malignant transformation • Cyst lined by epithelial lining • Lymphoid aggrgation
Warthin’s tumour • Columnar epithelium with lymphoid stroma • No malgnant transformation
Adenoid cystic carcinoma • Epithelial cell islands with microcystic change • Very locally infiltrative (especially around nerves) but metastasises late