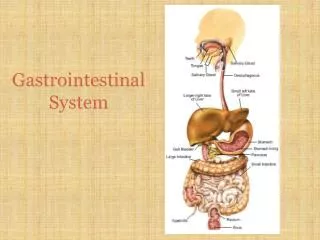
Gastrointestinal System Disorders
730 likes | 861 Vues
Explore various digestive conditions affecting the esophagus and stomach, from normal appearances to ulcers, cancers, gastritis, and more. Detailed medical images and descriptions included.

Gastrointestinal System Disorders
E N D
Presentation Transcript
This is a normal esophagus with the usual white to tan smooth mucosa seen at the left. Thegastroesophageal junction (not an anatomic sphincter) is at the center, and the stomach is at the right.
This is normal esophageal squamous mucosa at the left, with underlying submucosa. The muscularis is at the right.
This is Candida esophagitis. Tan-yellow plaques are seen in the lower esophagus, along with mucosal hyperemia. The same lesions are also seen at the upper right in the stomach.
Acute esophagitis is manifested here by infiltrating neutrophils to the squamous mucosa as well as submucosa.
The lower esophagus here shows sharply demarcated ulcerations that have a brown-red base, contrasted with the normal pale white esophageal mucosa at the far left.
An esophageal ulcer is seen here microscopically to have a sharp margins. The ulcer base at the left shows loss of overlying squamous epithelium with only necrotic debris remaining.
Here are two more sharply demarcated "punched out" ulcerations of the mid esophagus.
Barrett's esophagus in which there is gastric-type mucosa above the gastroesophageal junction. Note the columnar epithelium to the left and the squamous epithelium at the right.
At the lower end of the esophagus (which has been turned inside out at autopsy) are linear dark blue submucosal dilated veins known as varices. In patients with portal hypertension (usually secondary to liver cirrhosis from chronic alcoholism), the submucosal esophageal veins become dilated (form varices). These varices are prone to bleed.
Esophageal variceal bleeding. Here is another varix near the gastroesophageal junction that is dark red black because it has been bleeding. (The esophagus has been turned inside out.)
Inflammation and hemorrhage is seen here in the region of a ruptured varix of the esophagus.
This radiograph taken following barium swallow demontrates astricturein the lower esophagus, with pooling of the contrast above the point of stricture. Such stricture may complicate conditions such as scleroderma, gastroesophageal reflux disease, or carcinoma.
History of smoking and/or alcoholism is often present in patients with esophageal squamous carcinoma, while a history of Barrett's esophagus precedes development of esophageal adenocarcinoma in many cases. Here, an ill-defined mass at the gastroesophageal junction produces mucosal ulceration and irregularity, which led to the clinical symptoms of pain and difficulty swallowing.
This irregular reddish, ulcerated exophyticmid-esophageal massas seen on the mucosal surface is a squamous cell carcinoma..
At high power, these infiltrating nests of neoplastic cells have abundant pink cytoplasm and distinct cell borders typical for squamous cell carcinoma. Esophageal carcinomas are not usually detected early and, therefore, have a very poor prognosis.
This is the normal appearance of thegastric antrumextending to thepylorusat the right of center. Thefirst portion of the duodenum (duodenal bulb) is at the far right..
This is the normal appearance of the gastric fundal mucosa, with short pits lined by pale columnar mucus cells leading into long glands which contain bright pink parietal cells that secrete hydrochloric acid.
This is an acute gastritis with a diffusely hyperemic gastric mucosa. There are many causes for acute gastritis.
Here are some larger areas of gastric hemorrhage that could best be termed "erosions" because the superficial mucosa is eroded away. The findings here fit with acute erosive gastritis.
At high power, gastric mucosa demonstrates infiltration by neutrophils. This is acute gastritis
A 1 cm acute gastric ulcer is shown here in the upper fundus. The ulcer is shallow and sharply demarcated, with surrounding hyperemia. It is probably benign. However, all gastric ulcers should be biopsied to rule out a malignancy.
Here is a much larger 3 x 4 cm gastric ulcer that led to the resection of the stomach shown here. This ulcer is much deeper with more irregular margins. Complications of gastric ulcers (either benign or malignant) include pain, bleeding, perforation, and obstruction.
Microscopically, the ulcer here is sharply demarcated, with normal gastric mucosa on the left falling away into a deep ulcer whose base contains infamed, necrotic debris. An arterial branch at the ulcer base is eroded and bleeding.
Infection with Helicobacter pylori. This small curved to spiral rod-shaped bacterium is found in the surface epithelial mucus of most patients with active gastritis. The rods are seen here with a methylene blue stain.
Helicobacter pylori, gastric biopsy, silver stain on left, giemsa stain on right.
Helicobacter pylori • Causes 70% of gastric peptic ulcers • Causes 95% of duodenal peptic ulcers • Causes chronic gastritis • Causes gastric carcinomas • Causes MALT lymphomas
GASTRIC TUMORS • BENIGN • MALIGNANT
Gastric neoplasia is not uncommon. Here is a gastric adenocarcinoma. In the U.S., most gastric cancers are discovered at a late stage when the neoplasm has invaded and/or metastasized. ALL gastric ulcers and ALL gastric masses must be biopsied, because it is not possible to tell from gross appearance alone which are benign and which are malignant. In contrast, virtually all duodenal peptic ulcers are benign.
Here is a gastric ulcer in the center of the picture. It is shallow and is about 2 to 4 cm in size. This ulcer on biopsy proved to be malignant, so the stomach was resected as shown here.
At higher magnification, the neoplastic glands of gastric adenocarcinoma demonstrate mitoses, increased nuclear/cytoplasmic ratios, and hyperchromatism.
At high power, this gastric adenocarcinoma is so poorly differentiated that glands are not visible. Instead, rows of infiltrating neoplastic cells with marked pleomorphism are seen. Many of the neoplastic cells have clear vacuoles of mucin.
This is a signet ring cell pattern of adenocarcinoma in which the cells are filled with mucin vacuoles that push the nucleus to one side, as shown at the arrow.
This is the normal appearance of small intestinal mucosa with long villi that have occasional goblet cells. The villi provide a large area for digestion and absorption.
This is an adhesion between loops of small intestine. Such adhesions are typical following abdominal surgery. More diffuse adhesions may also form following peritonitis.
The dark red infarcted small intestine contrasts with the light pink viable bowel. This is one complication of adhesions from previous surgery. The trapped bowel has lost its blood supply.
The mucosal surface of the bowel seen here shows necrosis with hyperemia extending all the way through the mucosa. The submucosa and muscularis, however, are still intact.
At higher magnification with more advanced necrosis, the small intestinal mucosa shows hemorrhage with acute inflammation in this case.
Seen here at the ileocecal valve is a tumor that has a faint yellowish color. This is a carcinoid tumor.
The carcinoid tumor is seen here to be a discreet, though not encapsulated, mass of multiple nests of small blue cells in the submucosa.
At high magnification, the nests of carcinoid tumor have a typical endocrine appearance with small round cells having small round nuclei and blue cytoplasm.
This is a leiomyosarcoma of the small bowel. As with sarcomas in general, this one is big and bad.
Seen here is the most common congenital anomaly of the GI tract--a Meckel's diverticulum.