Enhancing NHS Access to NGS Resources with Firewall Solutions and Collaboration
This document discusses the collaborative efforts to improve access to Next Generation Sequencing (NGS) resources for NHS clinicians and researchers. It highlights challenges such as secure communication and data anonymization within NHS firewalls, featuring scenarios like the Shared Genomics Project in Manchester and Monte Carlo Treatment Planning in Cardiff. Solutions discussed involve establishing liaisons for deployments and the importance of policy agreements, including SLAs and MoUs. Future work includes expanding the use of NGS to foster collaboration across institutions while ensuring patient data protection.

Enhancing NHS Access to NGS Resources with Firewall Solutions and Collaboration
E N D
Presentation Transcript
Firewalls, NHS and other organisations’ access to NGS resourcesPresent: Steve Brewer (facilitator/scribe), Gagarine (Greg) Yaikhom, Gareth Smith, David Wallom (towards end to discuss future work)
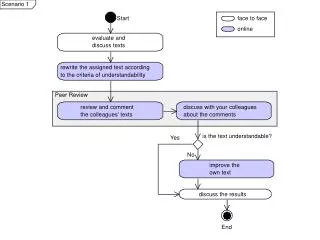
Scenario 1 • Gareth: Shared Genomics Project at Manchester – HPC analysis of large genomic datasets for patients. Providing infrastructure for clinicians and epidemiologists to do statistical analysis of genomic datasets coupled with medical data. (part social science/part bio-informatics). Local cluster with limited no. of users. (note: data already anonymised.) • Wider deployment throughout NHS could benefit a NGS job submission stack eg (RMCS). What will be required? Each deployment will require a liaison person
Scenario 2 • MCTP Monte Carlo Treatment Planning • Currently using Condor at Cardiff and accessing NGS resources at Oxford. • First challenge: clinicians and (perhaps) medical physicists want someone (or something) to sort out account registration and configuration. The tipping point is the language and new technologies (eg SSL) • Second challenge: establishing communication between secure networks such as the NHS and NGS. Default is firewall due to perceived security risk. MofU and/or SLAs needed. Patient data cannot leave the NHS firewall. NHS reluctant to allow the applications inside
Approaches • MCTP: anonymise patient data within NHS firewall, transfer to NGS, return o/p to NHS • Drawback – no standard anonymisation tool for radiotherapy; establishing connection difficult due to use of non-standard ports; conflict of different policy (NHS uses Caldicott rules/guidelines – NHS’s interpretation of data protection law) • Difficult to make progress untill both parties have policy agreements (MoU, SLA etc.) • NHS physicians currently using NGS system to run experiments. Other institutions are acquiring certificates and time – different process – could be streamlined
Future work • NGS is the glue that bridges between institutions. Shiboleth coming. How many NHS institutions are part of the UK Access management Federation. • See SARoNGS (Shibboleth Access to Resources on the National Grid Service )project. • David Wallom to help take forward both scenarios through NGS – solutions proposed • Precedent for MCTP in Genius project at UCL which runs real-time calculations of brain scans for surgeons during procedures. Data is transferred from NGS scanners to NGS and US TeraGrid.