Download
1 / 1
10 likes | 204 Vues
SPIRAL HEAD CT IN THE EVALUATION OF ACUTE INTRACRANIAL PATHOLOGY HEITOR OKANOBO MD, STEPHEN LEDBETTER MD MPH, AARON SODICKSON MD PhD EMERGENCY RADIOLOGY, BRIGHAM AND WOMEN ’ S HOSPITAL, HARVARD MEDICAL SCHOOL, BOSTON, MA. LEARNING OBJECTIVES:

E N D
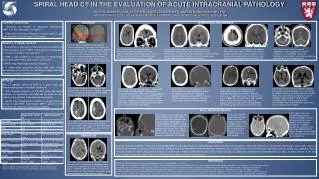
SPIRAL HEAD CT IN THE EVALUATION OF ACUTE INTRACRANIAL PATHOLOGY HEITOR OKANOBO MD, STEPHEN LEDBETTER MD MPH, AARON SODICKSON MD PhD EMERGENCY RADIOLOGY, BRIGHAM AND WOMEN’S HOSPITAL, HARVARD MEDICAL SCHOOL, BOSTON, MA LEARNING OBJECTIVES: 1. Recognize the benefits of multiplanar reformations (MPR’s) in the interpretation of head CT. 2. Understand technique differences of spiral head CT, and potential pitfalls of spiral head CT technique. TECHNIQUE INTRACRANIAL HEMORRHAGE BENEFITS OF SPIRAL HEAD CT: 1. As anatomy or pathology is often best demonstrated in an orthogonal plane, coronal MPR’s often enhance visualization of structures parallel to the axial plane.1,2 2. MPR’s add confidence in localization of hemorrhage, particularly at the vertex, tentorium, or parafalcine.3 3. MPR’s may better depict calvarial fractures.4 4. A single spiral acquisition of the head often allows retrospective reconstruction of maxillofacial images, and may eliminate the need for repeat scanning.5,6 Fig 1: a) Typical imaging planes for spiral & sequential technique. Red lines are straight axial gantry angle of spiral CT, yellow are gantry angled parallel to skull base for sequential scan. B) The head can be tilted forward in patients able to flex their neck, to eliminate posterior fossa beam hardening artifact, and to better approximate the acquisition plane of sequential head CT technique. Fig 5: Spiral scan a) in a trauma patient demonstrates either parenchymal of focal subarachnoid frontal hemorrhage (red). Coronal MPR b) confirms post-traumatic subarachnoid hemorrhage confined to the sulcus (yellow). Fig 6: Spiral scan a) demonstrates subtle parafalcine hyperdensity (red), possibly subarachnoid or subdural hemorrhage, vs thickened dura or meningioma. Coronal MPR b) reveals acute angulation and extension into adjacent sulcus (yellow), confirming subarachnoid hemorrhage. Fig 7: Spiral scan a) demonstrates thin subdural hematoma (red). Coronal MPR b) better depicts anatomic extent over the vertex (yellow), permits more accurate measurement of thickness, and reveals associated effacement of parietal sulci. Fig 8: Spiral scan a) reveals tentorial hyperdensity (red) suspicious for subdural hematoma. Coronal MPR b) shows the hematoma (blue) to better advantage by depicting the tentorium in an orthogonal plane. PITFALLS: Most CT gantries cannot be tilted for a spiral scan, and remain perpendicular to the table, resulting in: 1. More frequent inclusion of the skull base and dental hardware. To avoid this, the head can be tilted (in non-trauma) or the posterior fossa scanned sequentially. 2. Lesions may change position relative to a sequential scan (similar to axial MRI). Axial-oblique MPR’s parallel to the skull base can reproduce sequential positioning. Fig 2: Dental hardware artifact obscures the posterior fossa in spiral scan a). Repeat sequential scan b) through the posterior fossa with a tilted gantry angle eliminates the artifact. Fig 12: Spiral scan for trauma identifies infarction as the likely cause of the patient's fall. Axial image a) suggests subtle loss of grey-white differentiation (red), versus asymmetric positioning or volume averaging. Coronal MPR b) confirms early infarction (yellow), with loss of grey-white differentiation, and sulcal effacement, better seen in cross-section to the anatomy. Fig 11: Spiral scan a) in a patient with prior glioblastoma multiforme resection reveals unchanged post-operative subdural collection (green, prior imaging not shown), and diffuse white matter hypodensity crossing midline (red). Coronal MPR b) shows extension across the corpus callosum (yellow), confirmed on subsequent MRI (not shown) to represent interval tumor extension. Fig 9: Spiral scan in a trauma patient a) reveals right frontal scalp laceration (green), and small right parafalcine hyperdensity (red), either a small subdural hematoma or a meningioma. On coronal MPR b), the lesion has a smooth, rounded contour with a broad dural base, suggesting meningioma. MRI (not shown) confirmed a homogeneously enhancing lesion with a dural tail consistent with meningioma. Fig 10: Spiral CT in a trauma patient a) demonstrates rounded hyperdensity (red) at the right parietal convexity, suggesting subdural hematoma. Coronal MPR b) reveals adjacent hyperostosis (yellow) of the inner calvarial table consistent with meningioma. SKULL AND MAXILLOFACIAL Fig 15: Spiral scan after transphenoidal pituitary adenoma resection a). Sella turcica evaluation is often limited in the axial plane, although an amorphous hypodensity is present in the sella (red). Sagittal MPR b) depicts the bony defect (yellow) in the sella floor and sphenoid sinus fat packing. Fig 14: Coronal MPR demonstrates parietal fracture (red) and diastasis (yellow) of the lambdoid suture a). We would like to offer you a job if you could have found the fracture prospectively on the axial image b). Fig 13: Spiral scan a) reveals postero-lateral maxillary sinus wall fracture (red), and segmental zygomatic arch fractures (yellow). Spiral acquisition enabled retrospective MPR’s without the need to bring the patient back for a dedicated maxillofacial scan. Sagittal MPR b) shows clinically unsuspected right orbital floor fracture (blue) not previously detected on axial images. Fig 3: Apparent change in hematoma position from spiral a) & sequential b) scans due to different acquisition angle. Spiral scans can be reformatted to angled axial-oblique MPR’s parallel to the skull base to simulate sequential positioning. HERNIATION CONCLUSION Spiral CT technique enables routine use of high quality MPR’s, and has become our standard approach for all head trauma patients. Improved evaluation of intracranial hemorrhage, mass effect, skull and maxillofacial fractures are among its many benefits. Although one must be aware of potential technical limitations (e.g. streak artifact in the posterior fossa) and interpretational pitfalls (e.g., apparent change in location of lesions) when using spiral technique, its routine use in head trauma patients can increase visual conspicuity, diagnostic confidence and interpretational accuracy. In select patients, it can also reduce radiation exposure and provide for more efficient and timely provision of patient care. REFERENCES 1. Mirvis SE, Shanmuganagthan K. Imaging hemidiaphragmatic injury. Eur Radiol 2007; 17:1411-1421. 2. Jayashankar A, Udayasankar U, Sebastian S, et al. MDCT of thoraco-abdominal trauma: an evaluation of the success and limitations of primary interpretation using MPR’s vs axial images. Emerg Radiol 2008; 15:29-34. 3. Strub WM, Leach JL, Tomsick T, Vagal A. Overnight preliminary head CT interpretations provided by residents: locations of misidentified intracranial hemorrhage. AJNR Am J Neuroradiol 2007; 28:1679-1682. 4. Hofman PA, Nelemans P, Kemerink GJ, Wilmink JT. Value of radiological diagnosis of skull fracture in the management of mild head injury: meta-analysis. J Neurol Neurosurg Psychiatry 2000; 68:416-422. 5. Turner BG, Rhea JT, Thrall JH, Small AB, Novelline RA. Trends in the use of CT and radiography in the evaluation of facial trauma, 1992-2002: implications for current costs. AJR Am J Roentgenol 2004; 183:751-754. 6. Ptak T, Rhea JT, Novelline RA. Radiation dose is reduced with a single-pass whole-body MDCT trauma protocol compared with a conventional segmented method: initial experience. Radiology 2003; 229:902-905.0 Fig 4: Spiral scan a) of right hemispheric subdural hematoma, with effaced right quadrigeminal plate cistern (red) and midline shift. Coronal MPR better depicts isodense subdural hematoma extent (blue), permits better size measurement, and directly shows uncus herniation over the tentorium (green). Table 1: Sequential & Spiral head CT protocol technical parameters 1 Based on detector configuration options on Siemens Somatom Sensation 64 2 CTDI = CT Dose Index, DLP = Dose Length Product (from the included cases)